

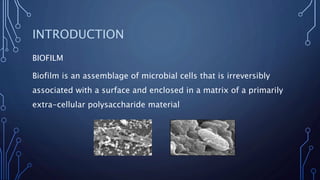

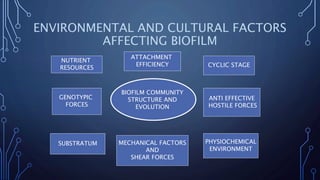







This document summarizes key information about fungal biofilms. It discusses how biofilms are formed through distinct developmental phases. Biofilms are composed of microbial cells embedded in an extracellular matrix that provides structure and protects cells. Many medically important fungi like Candida, Aspergillus, and Cryptococcus can form biofilms. Biofilms contribute to infections associated with medical devices and are highly resistant to antifungal treatments. The formation and structure of fungal biofilms is regulated by complex genetic and environmental factors.
































![Characteristics of Bacterial Biofilm(Edited) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/characteristicsofbacterialbiofilmeditedautosaved-260128100342-faceed21-thumbnail.jpg?width=640&height=640&fit=bounds)






















































