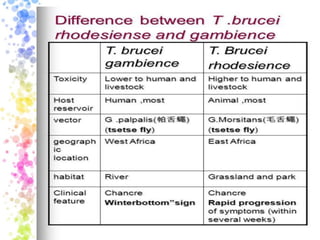
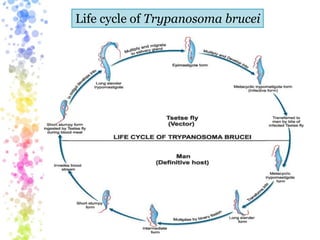
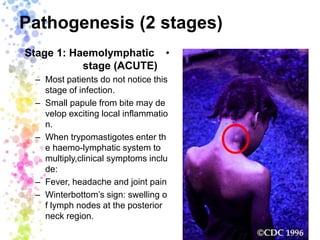
The document provides an overview of African trypanosomiasis, also known as sleeping sickness, caused by the parasite Trypanosoma brucei and transmitted by the tsetse fly, highlighting its significant public health impact in sub-Saharan Africa. It describes the life cycle, transmission modes, and two stages of pathogenesis of T. brucei, along with preventive measures including insecticide use and early diagnosis. Additionally, it covers American trypanosomiasis or Chagas disease caused by Trypanosoma cruzi, its transmission via kissing bugs and domestic animals, and the different clinical manifestations in acute and chronic phases.



![Trypanosoma [1]](https://cdn.slidesharecdn.com/ss_thumbnails/trypanosomaseminar1-170312074241-thumbnail.jpg?width=640&height=640&fit=bounds)































































