Downloaded 970 times

































![Acid-Base Physiology
• pH is the negative logarithm to the base 10 of the hydrogen ion
concentration in mmol/L
• pH = - log10[H+]
• An increase in pH indicates a proportionate decrease in the [H+] and
a decrease in the pH indicates a proportionate increase in the [H+].
• H2CO3 generates 12,500 mmol H+ per day.
• Normal metabolism of proteins and nucleotides generates about 100
mmol H+ per day in the form of sulphuric and phosphoric acids.](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-38-2048.jpg)











![Characteristics of acid-base disorders
DISORDER PRIMARY RESPONSES COMPENSATORY
RESPONSE
Metabolic
acidosis
[H+] PH HCO3
- pCO2
Metabolic
alkalosis
[H+] PH HCO3
- pCO2
Respiratory
acidosis
[H+] PH pCO2 HCO3
-
Respiratory
alkalosis
[H+] PH pCO2 HCO3
-](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-50-2048.jpg)
![Prediction of compensation
Metabolic acidosis PaCO2= (1.5 x HCO3
-) + 8 ± 2
Metabolic alkalosis
PaCO2 will↑ 0.75 mmHg per
mmol/L ↑ in [HCO3
-]
Respiratory
acidosis
Acute
[HCO3
-] will ↑ 0.1 mmol/L per
mmHg in PaCO2
Chronic
[HCO3
-] will ↑ 0.4 mmol/L per
mmHg in PaCO2
Respiratory
alkalosis
Acute
[HCO3
-] will ↑ 0.2 mmol/L per
mmHg in PaCO2
Chronic
[HCO3
-] will ↑ 0.4 mmol/L per
mmHg in PaCO2](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-51-2048.jpg)

![• Albumin is the major unmeasured anion
• The anion gap should be corrected if there are
gross changes in serum albumin levels.
AG (CORRECTED) = AG + { (4 – [ALBUMIN]) × 2.5}](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-53-2048.jpg)


![PLASMA OSMOLAR GAP
Calculated Plasma Osmolarity = 2[Na+] + [Gluc]/18 +
[BUN]/2.8
Normal Measured Plasma Osmolarity > Calculated
Plasma Osmolarity (upto 10 mOsm/L)
Measured Plasma Osmolarity - Calculated Plasma
Osmolarity > 10 mOsm/kg indicates presence of abnormal
osmotically active substance
Ethanol
Methanol
Ethylene glycol](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-56-2048.jpg)
![URINARY ANION GAP
• Urinary NH4
+ levels can be estimated by calculating the
urine anion gap (UAG)
• UAG = [Na+ + K+]u – [Cl–]u
• [Cl–]u > [Na+ + K+], the urine gap is negative by definition
• Helps to distinguish GI from renal causes of loss of
HCO3 by estimating Urinary NH4+ (elevated in GI HCO3
loss but low in distal RTA).
• Hence a -ve UAG (av -20 meq/L) seen in former while
+ve value (av +23 meq/L) seen in latter.](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-57-2048.jpg)





















![pH is inversely related to [H+]; a pH change of 1.00
represents a 10-fold change in [H+]
pH [H+] in nanomoles/L
7.00 100
7.10 80
7.30 50
7.40 40
7.52 30
7.70 20
8.00 10
Relation b/w pH & H+ conc.
Assessment of validity of test results](https://image.slidesharecdn.com/abg-final-151206120252-lva1-app6891/75/ARTERIAL-BLOOD-GAS-ANALYSIS-79-2048.jpg)



















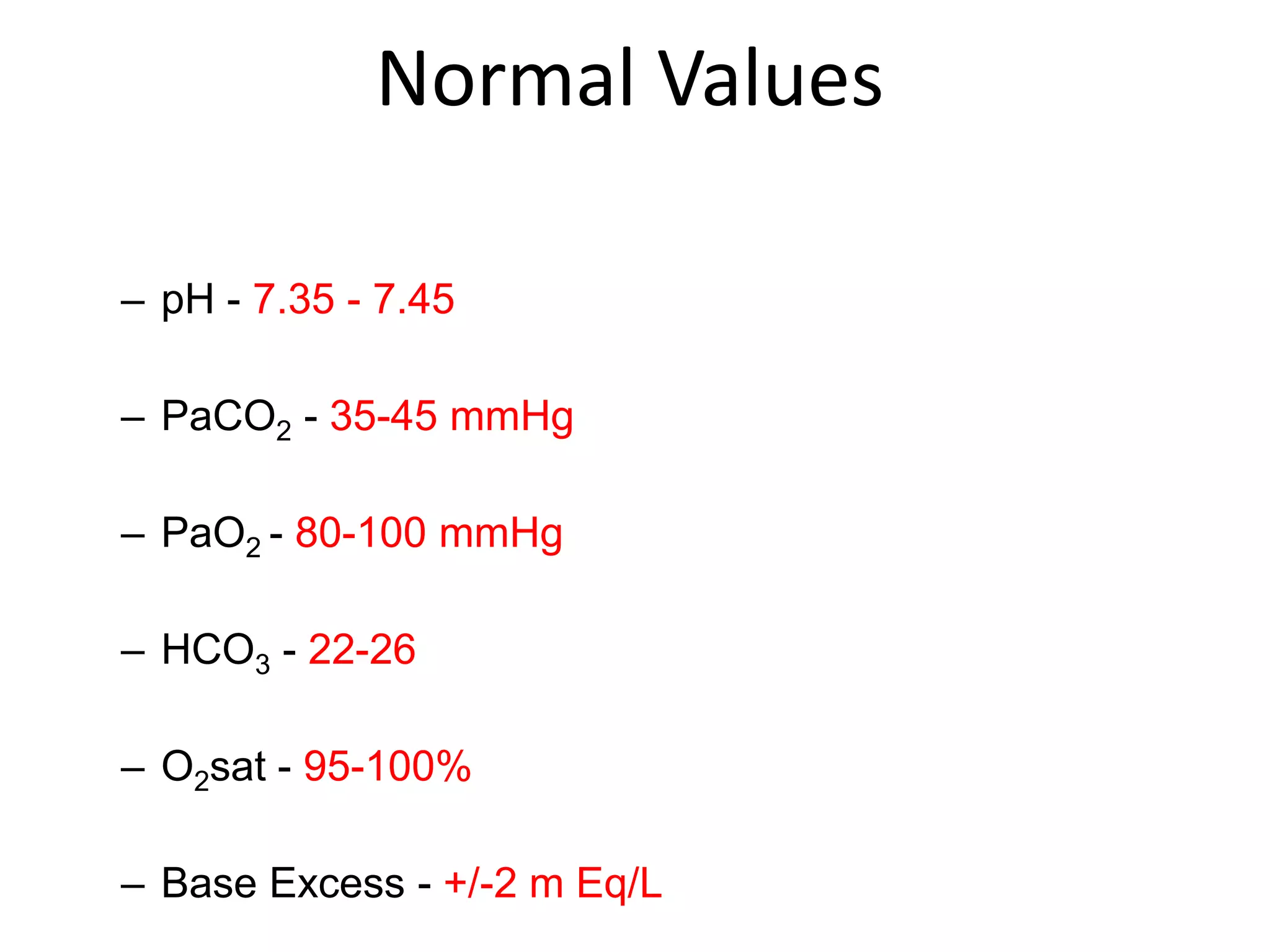
This document provides information about arterial blood gas (ABG) analysis. It defines an ABG as a blood sample drawn from an artery to assess acid-base balance, oxygenation, and ventilation. ABGs are ordered to diagnose and monitor respiratory failure and changes in acid-base homeostasis. The components of an ABG include pH, PaCO2, PaO2, HCO3, O2 saturation, and base excess. Normal values for these components are provided. The document discusses how to properly collect an ABG sample and handle it to avoid inaccurate results. It also covers acid-base physiology and the four primary acid-base disorders: metabolic acidosis, metabolic alkalosis, respiratory acidosis, and respiratory alk

















































![ABG[1].pptx BY DR BHAWNA ESI PGIMSR, BASAIDA](https://cdn.slidesharecdn.com/ss_thumbnails/abg1-250915145144-de471f3c-thumbnail.jpg?width=640&height=640&fit=bounds)















































