Downloaded 47 times

![Acid-Base Physiology
• pH is the negative logarithm to the base 10 of the hydrogen ion
concentration in mmol/L
• pH = - log10[H+]
• An increase in pH indicates a proportionate decrease in the [H+] and a
decrease in the pH indicates a proportionate increase in the [H+].
• H2CO3 generates 12,500 mmol H+ per day.
• Normal metabolism of proteins and nucleotides generates about 100
mmol H+ per day in the form of sulphuric and phosphoric acids.@ NKMishra23/07/18 4](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-4-2048.jpg)

















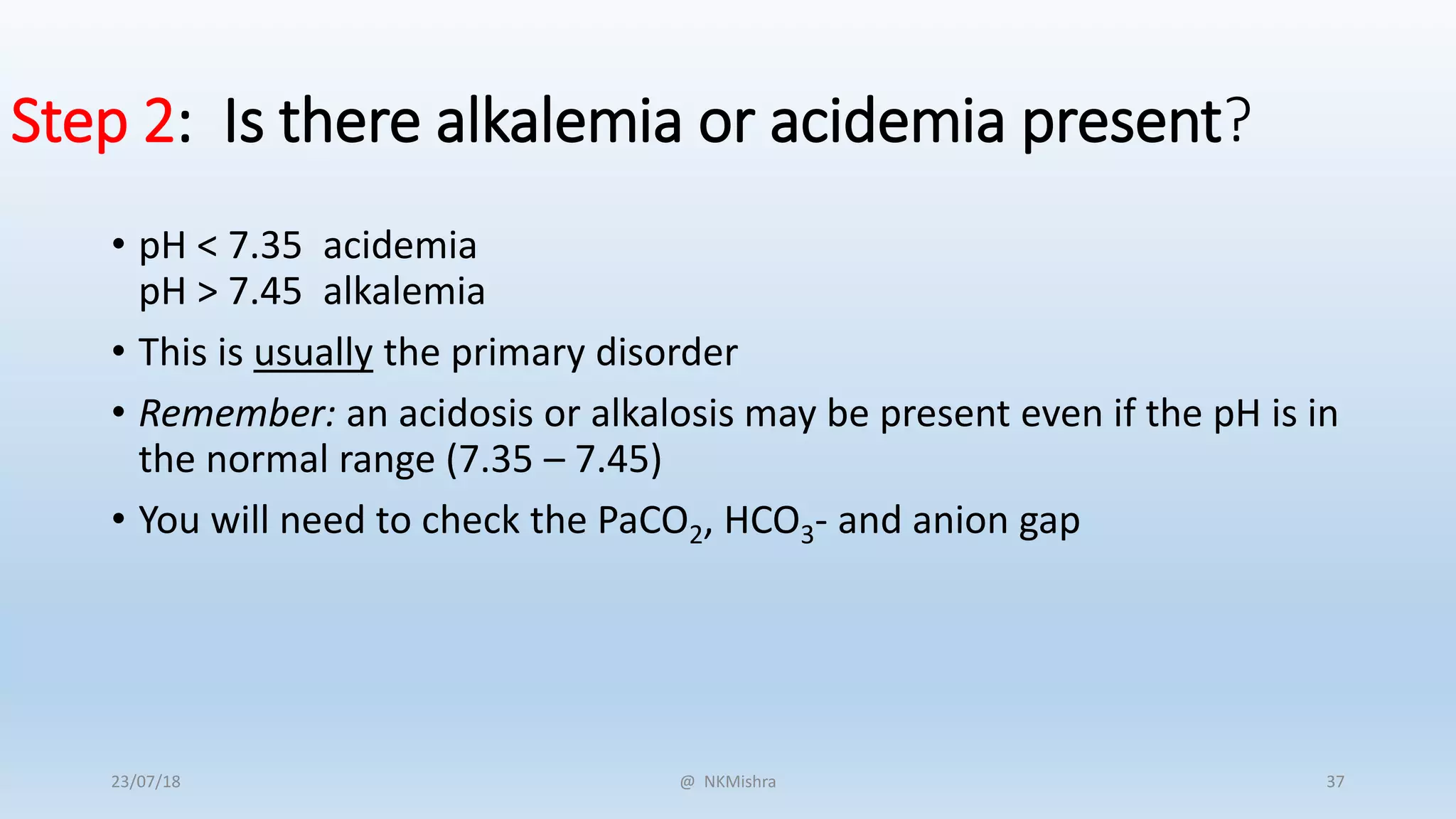
![Step 1: Assess the internal consistency of the values using
the Henderseon-Hasselbach equation:
• [H+] = 24(PaCO2)
[HCO3-]
@ NKMishra23/07/18 35](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-34-2048.jpg)
![pH Approximate [H+]
(mmol/L)
7.00 100
7.05 89
7.10 79
7.15 71
7.20 63
7.25 56
7.30 50
7.35 45
7.40 40
7.45 35
7.50 32
7.55 28
7.60 25
7.65 22
If the pH and the [H+] are inconsistent, the ABG is probably not valid.
@ NKMishra23/07/18 36](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-35-2048.jpg)

![• Step 4: Is there appropriate compensation for the primary disturbance?
• Usually, compensation does not return the pH to normal (7.35 – 7.45) except….?
Disorder Expected compensation Correction factor
Metabolic acidosis PaCO2 = (1.5 x [HCO3-]) +8 ± 2
Acute respiratory acidosis Increase in [HCO3-]= ∆ PaCO2/10 ± 3
Chronic respiratory acidosis (3-5 days) Increase in [HCO3-]= 3.5(∆ PaCO2/10)
Metabolic alkalosis Increase in PaCO2 = 40 + 0.6(∆HCO3-)
Acute respiratory alkalosis Decrease in [HCO3-]= 2(∆ PaCO2/10)
Chronic respiratory alkalosis Decrease in [HCO3-] = 5(∆ PaCO2/10) to 7(∆
PaCO2/10)
If the observed compensation is not the expected compensation, it is likely that more than one acid-base disorder is
present. @ NKMishra23/07/18 39](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-38-2048.jpg)
![• Step 5: Calculate the anion gap (if a metabolic acidosis exists):
• AG= [Na+]-( [Cl-] + [HCO3-] )=12 ± 2
• A normal anion gap is approximately 12 meq/L.
• In patients with hypoalbuminemia, the normal anion gap is lower than 12 meq/L; the
“normal” anion gap in patients with hypoalbuminemia is about 2.5 meq/L lower for
each 1 gm/dL decrease in the plasma albumin concentration (for example, a patient
with a plasma albumin of 2.0 gm/dL would be approximately 7 meq/L.)
• If the anion gap is elevated, consider calculating the osmolal gap in compatible clinical
situations.
• Elevation in AG is not explained by an obvious case (DKA, lactic acidosis, renal failure
• Toxic ingestion is suspected
• OSM gap = measured OSM – (2[Na+] - glucose/18 – BUN/2.8
• The OSM gap should be < 10
@ NKMishra23/07/18 40](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-39-2048.jpg)
![• Step 6: If an increased anion gap is present, assess the relationship between
the increase in the anion gap and the decrease in [HCO3-].
• Assess the ratio of the change in the anion gap (∆AG ) to the change in [HCO3-
] (∆[HCO3-]): ∆AG/∆[HCO3-]
• This ratio should be between 1.0 and 2.0 if an uncomplicated anion gap
metabolic acidosis is present.
• If this ratio falls outside of this range, then another metabolic disorder is
present:
• If ∆AG/∆[HCO3-] < 1.0, then a concurrent non-anion gap metabolic acidosis is
likely to be present.
• If ∆AG/∆[HCO3-] > 2.0, then a concurrent metabolic alkalosis is likely to be
present.
• It is important to remember what the expected “normal” anion gap for your
patient should be, by adjusting for hypoalbuminemia (see Step 5, above.)
@ NKMishra23/07/18 41](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-40-2048.jpg)
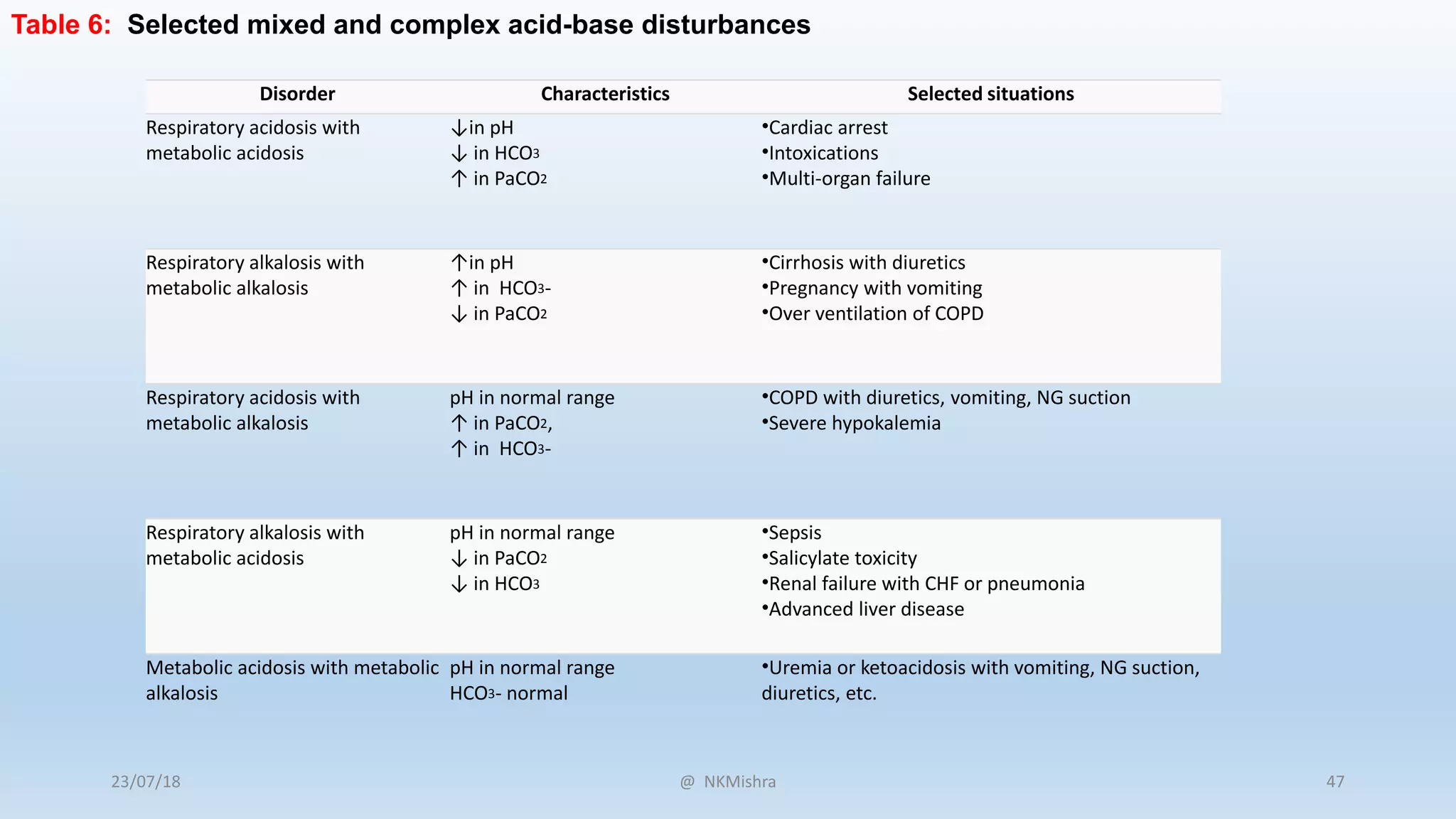
![Disorder pH Primary problem Compensation
Metabolic acidosis ↓ ↓ in HCO3- ↓ in PaCO2
Metabolic alkalosis ↑ ↑ in HCO3- ↑ in PaCO2
Respiratory acidosis ↓ ↑ in PaCO2 ↑ in [HCO3-]
Respiratory alkalosis ↑ ↓ in PaCO2 ↓ in [HCO3-]
Table 1: Characteristics of acid-base disturbances
@ NKMishra23/07/18 42](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-41-2048.jpg)

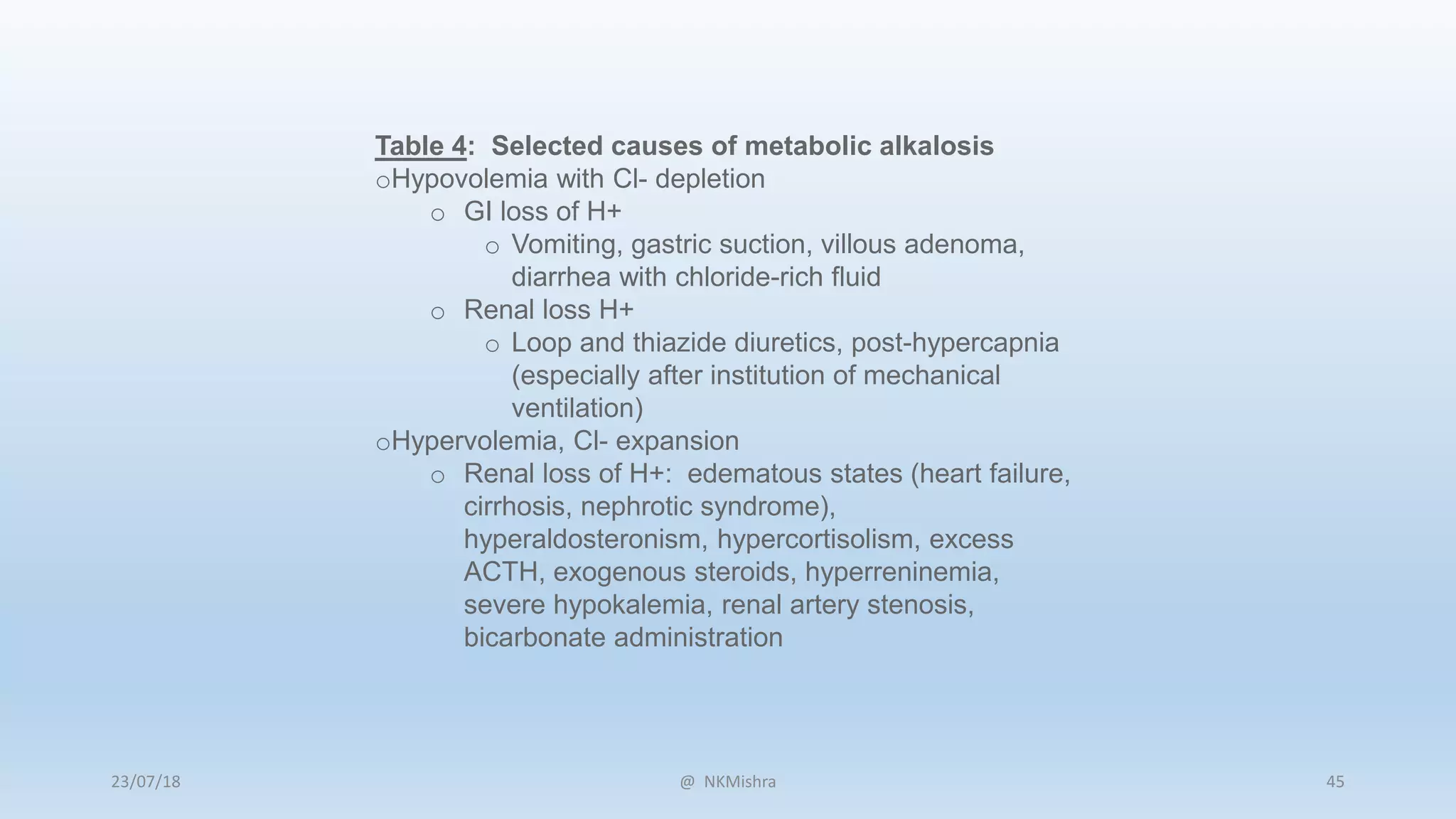
![Table 5: Selected etiologies of metabolic acidosis
oElevated anion gap:
o Methanol intoxication
o Uremia
o Diabetic ketoacidosisa, alcoholic ketoacidosis,
starvation ketoacidosis
o Paraldehyde toxicity
o Isoniazid
o Lactic acidosisa
o Type A: tissue ischemia
o Type B: Altered cellular metabolism
o Ethanolb or ethylene glycolb intoxication
o Salicylate intoxication
a Most common causes of metabolic acidosis with an
elevated anion gap
b Frequently associated with an osmolal gap
oNormal anion gap: will have increase in [Cl-]
o GI loss of HCO3-
o Diarrhea, ileostomy, proximal colostomy,
ureteral diversion
o Renal loss of HCO3-
o proximal RTA
o carbonic anhydrase inhibitor (acetazolamide)
o Renal tubular disease
o ATN
o Chronic renal disease
o Distal RTA
o Aldosterone inhibitors or absence
o NaCl infusion, TPN, NH4+ administration
@ NKMishra23/07/18 46](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-45-2048.jpg)


















![URINE ANION GAP
[Na+] + [K+] + [NH4
+] + [UC] ≈ [Cl-] + [HCO3-] + [UA]
[Na+] + [K+] - [Cl-] ≈ [UA] - [UC]
UAG ≈ [Na+] + [K+] - [Cl-]
?
@ NKMishra23/07/18 68](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-67-2048.jpg)
![HOW TO USE IT
NORMAL RESPONSE TO ACIDOSIS
UAG ≈ [Na+] + [K+] - [Cl-]
UAG < 0
IF KIDNEYS UNABLE TO EXCRETE H+
UAG ≈ [Na+] + [K+] - [Cl-]
UAG > 0
NH4
+ Cl- NH4
+ Cl
-
@ NKMishra23/07/18 69](https://image.slidesharecdn.com/abgatsbhu-190215185418/75/Approach-to-ABG-Analysis-68-2048.jpg)

























































































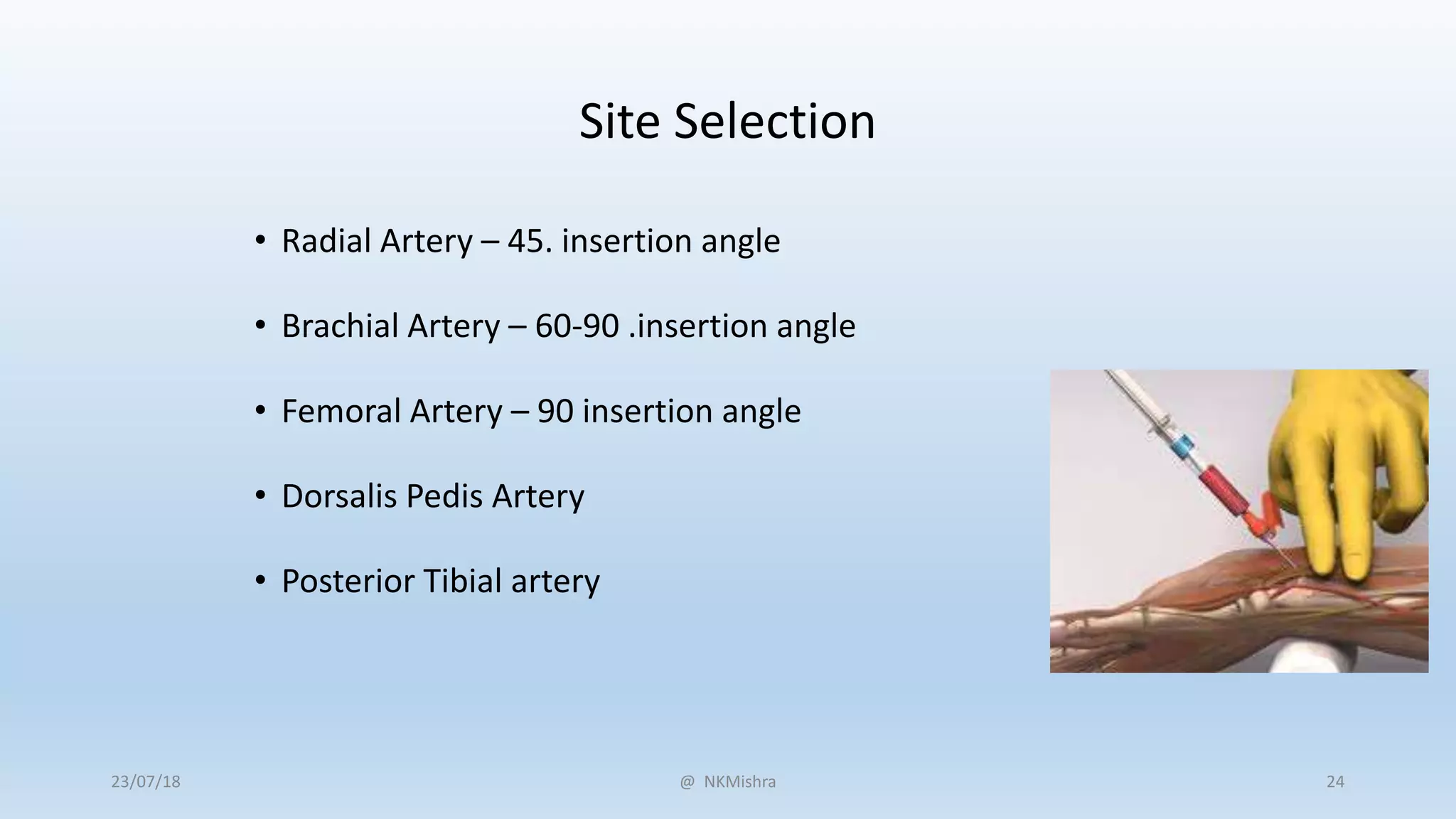
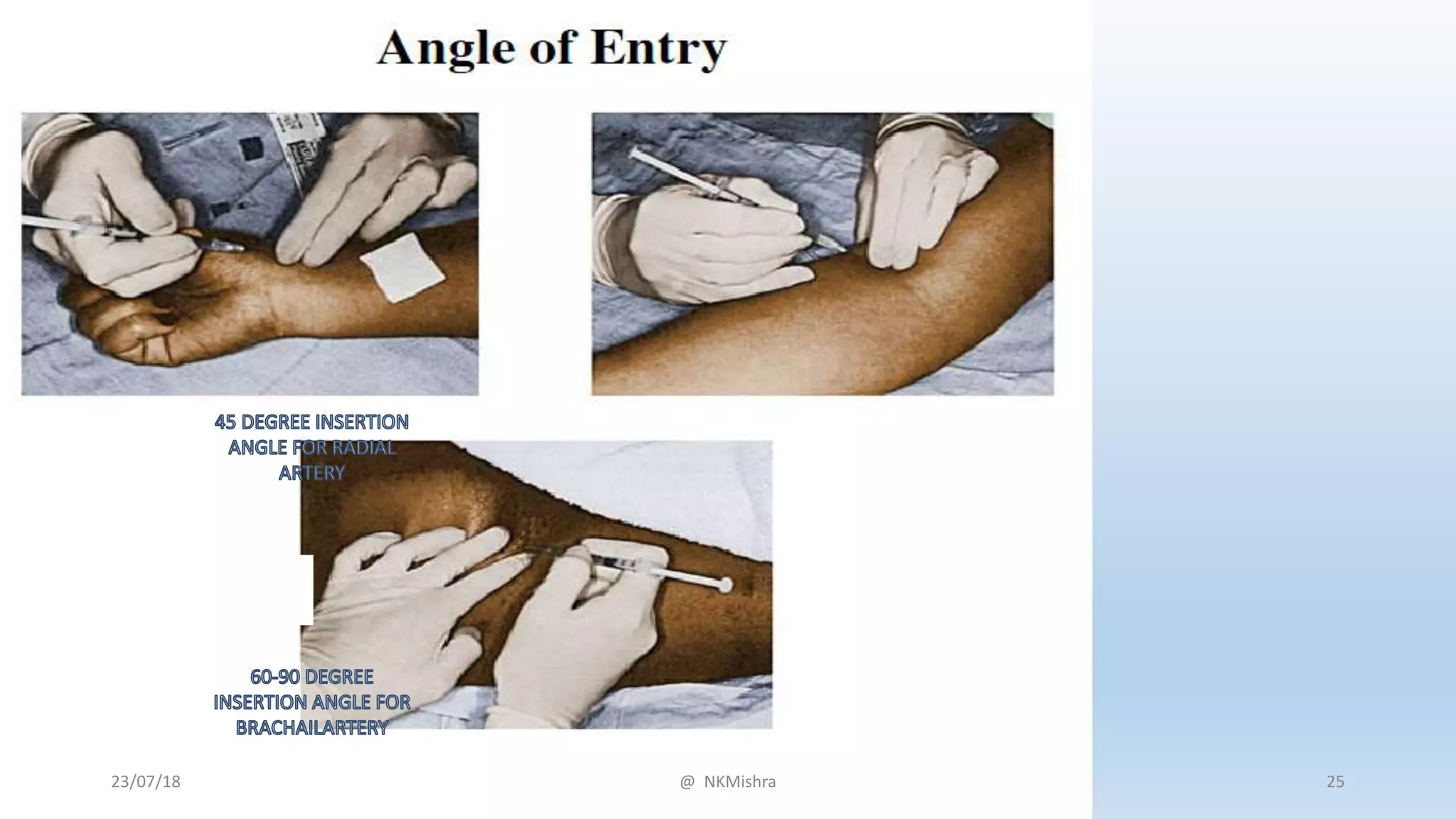
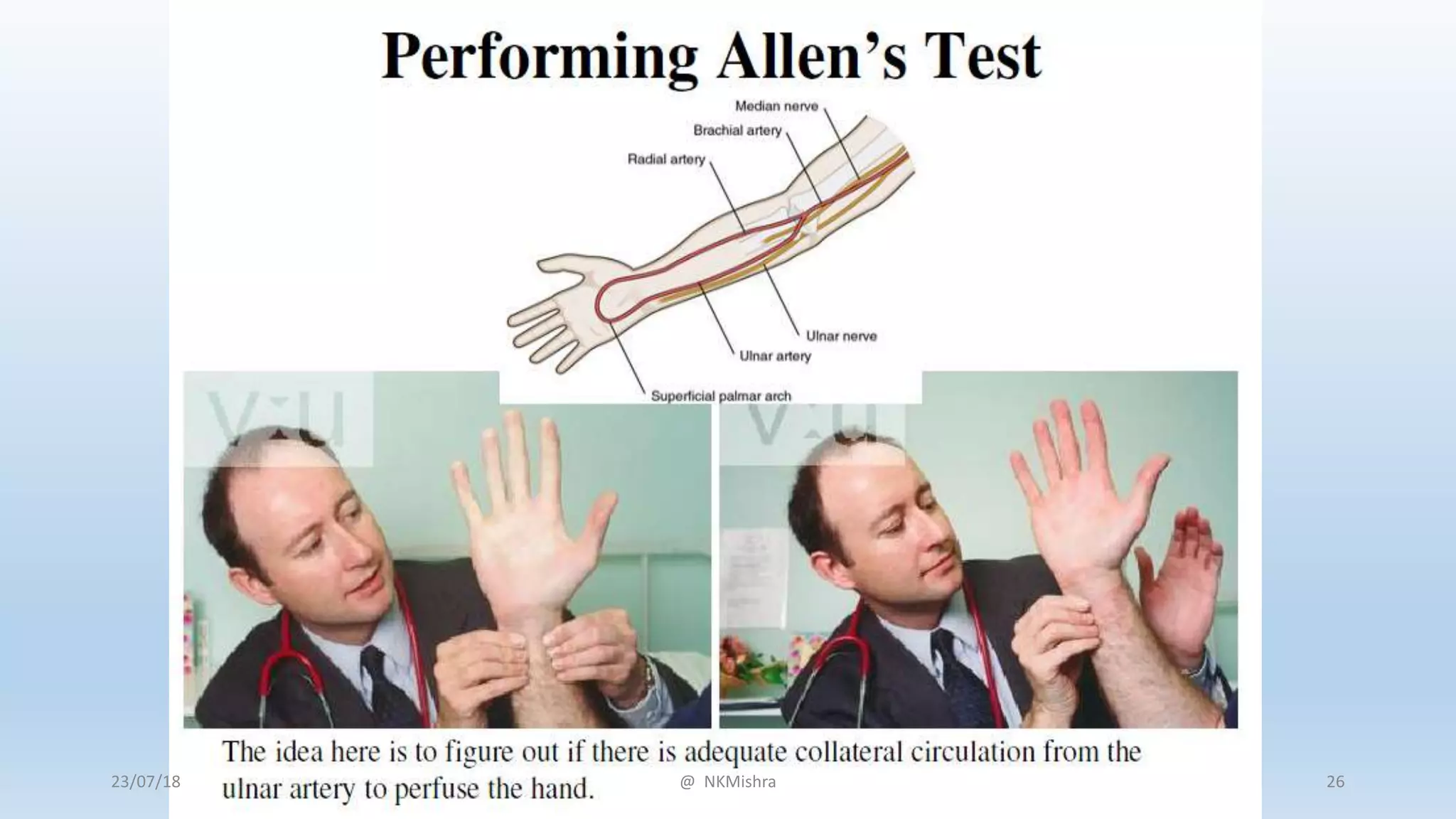
The document provides information on arterial blood gases (ABG), including the basics and interpretation of ABG results. It discusses key points such as the regulation of pH and factors involved in acid-base balance. Causes of acid-base disturbances like respiratory acidosis, respiratory alkalosis, metabolic acidosis and metabolic alkalosis are summarized. Technical aspects of ABG sampling and a stepwise approach to interpreting ABG results are also outlined in the document.


























![[Int. med] dyspnoea](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144320-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)








































