Downloaded 247 times
![INCLUSION CRITERIA
New York Heart Association (NYHA) class II, III, or IV symptoms, and
an ejection fraction of 40% or less (which was changed to 35% or less
by an amendment to the protocol on December 15, 2010).
Patients were required to have a plasma B-type natriuretic peptide
(BNP) level of at least 150 pg per milliliter (or an N-terminal pro-BNP
[NT-proBNP] level ≥600 pg per milliliter)
or
if they had been hospitalized for heart failure within the previous 12
months, a BNP of at least 100 pg per milliliter (or an NT-proBNP ≥400
pg per milliliter).](https://image.slidesharecdn.com/paradigm-hf-140928031738-phpapp01/75/Paradigm-hf-journal-club-presentation-4-2048.jpg)
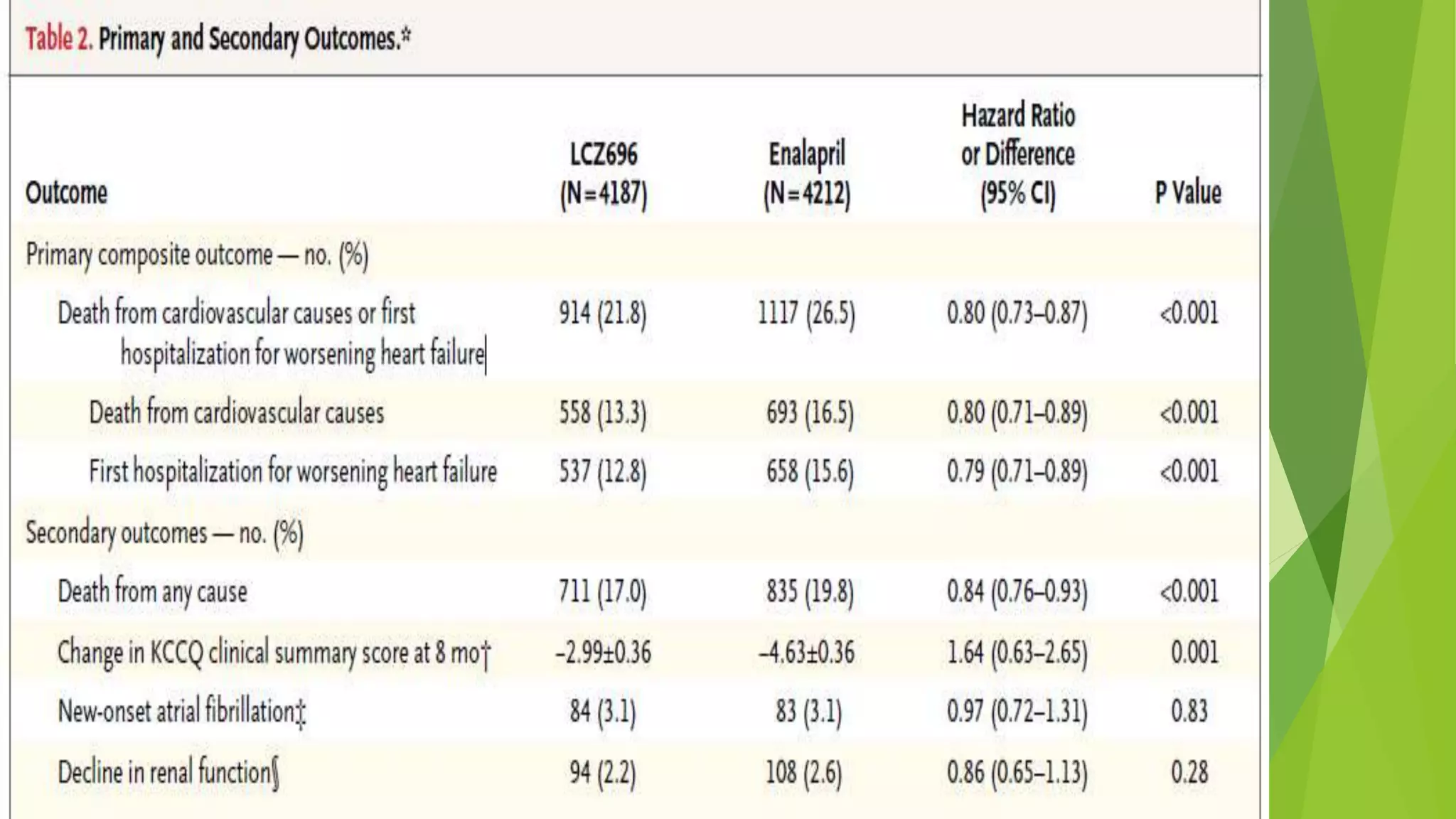
![Results:
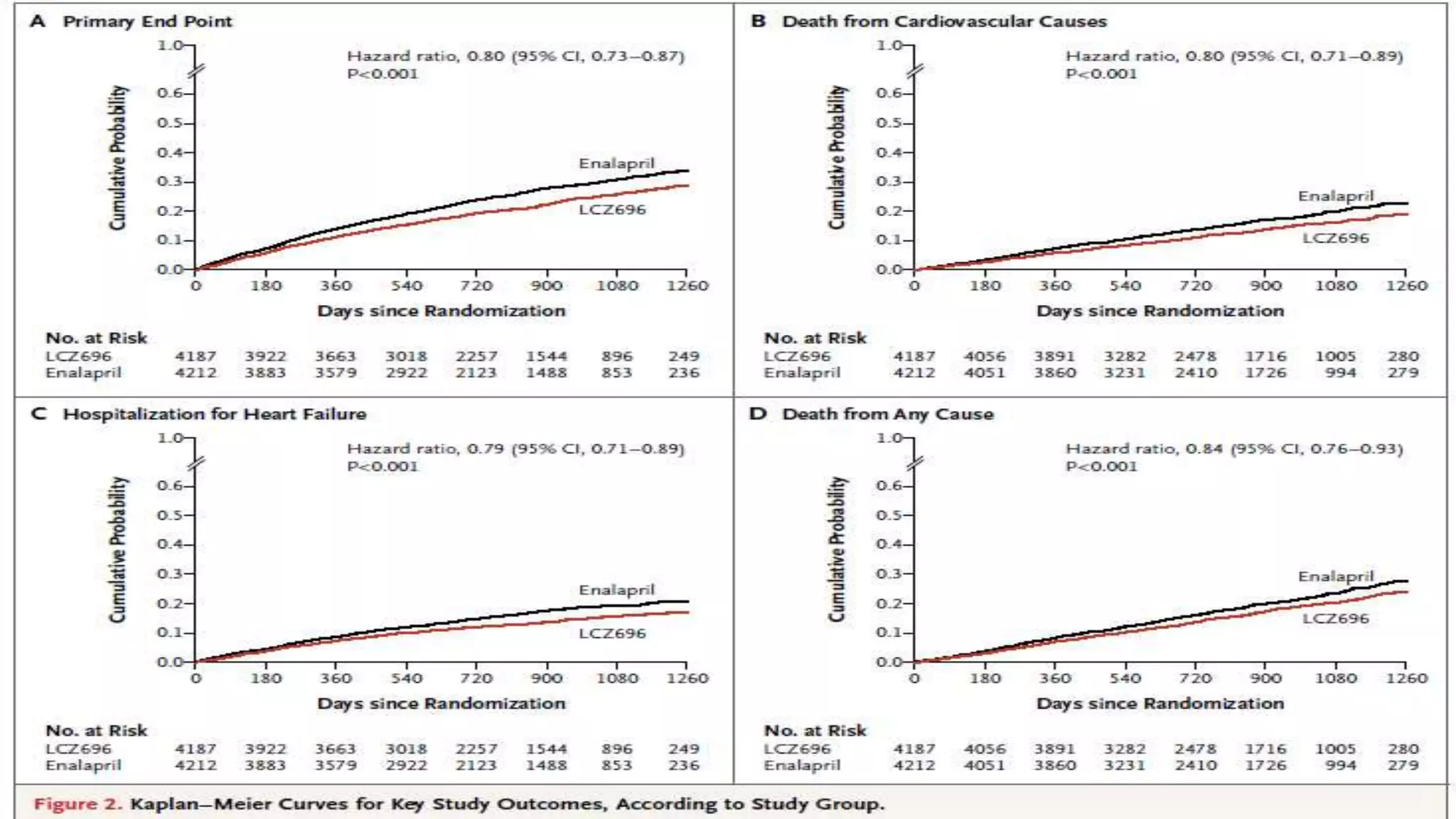
1. Primary outcome had occurred in 914 patients (21.8%) in the LCZ696 group and
1117 patients (26.5%) in the enalapril group (hazard ratio in the LCZ696 group,
0.80; 95% confidence interval [CI], 0.73 to 0.87; P<0.001).
2. A total of 711 patients (17.0%) receiving LCZ696 and 835 patients (19.8%)
receiving enalapril died (hazard ratio for death from any cause, 0.84; 95% CI, 0.76
to 0.93; P<0.001).
3. The trial was stopped early, according to prespecified rules, after a median follow
up of 27 months](https://image.slidesharecdn.com/paradigm-hf-140928031738-phpapp01/75/Paradigm-hf-journal-club-presentation-9-2048.jpg)

This randomized controlled trial compared the angiotensin receptor-neprilysin inhibitor LCZ696 to enalapril in over 8,400 patients with heart failure and reduced ejection fraction. It found that LCZ696 reduced the primary composite outcome of cardiovascular death or heart failure hospitalization by 20% compared to enalapril, as well as reducing overall mortality, cardiovascular mortality, heart failure hospitalizations, and improving symptoms. LCZ696 resulted in more hypotension and angioedema but less renal impairment, hyperkalemia, and coughing than enalapril.




















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)








