Downloaded 120 times
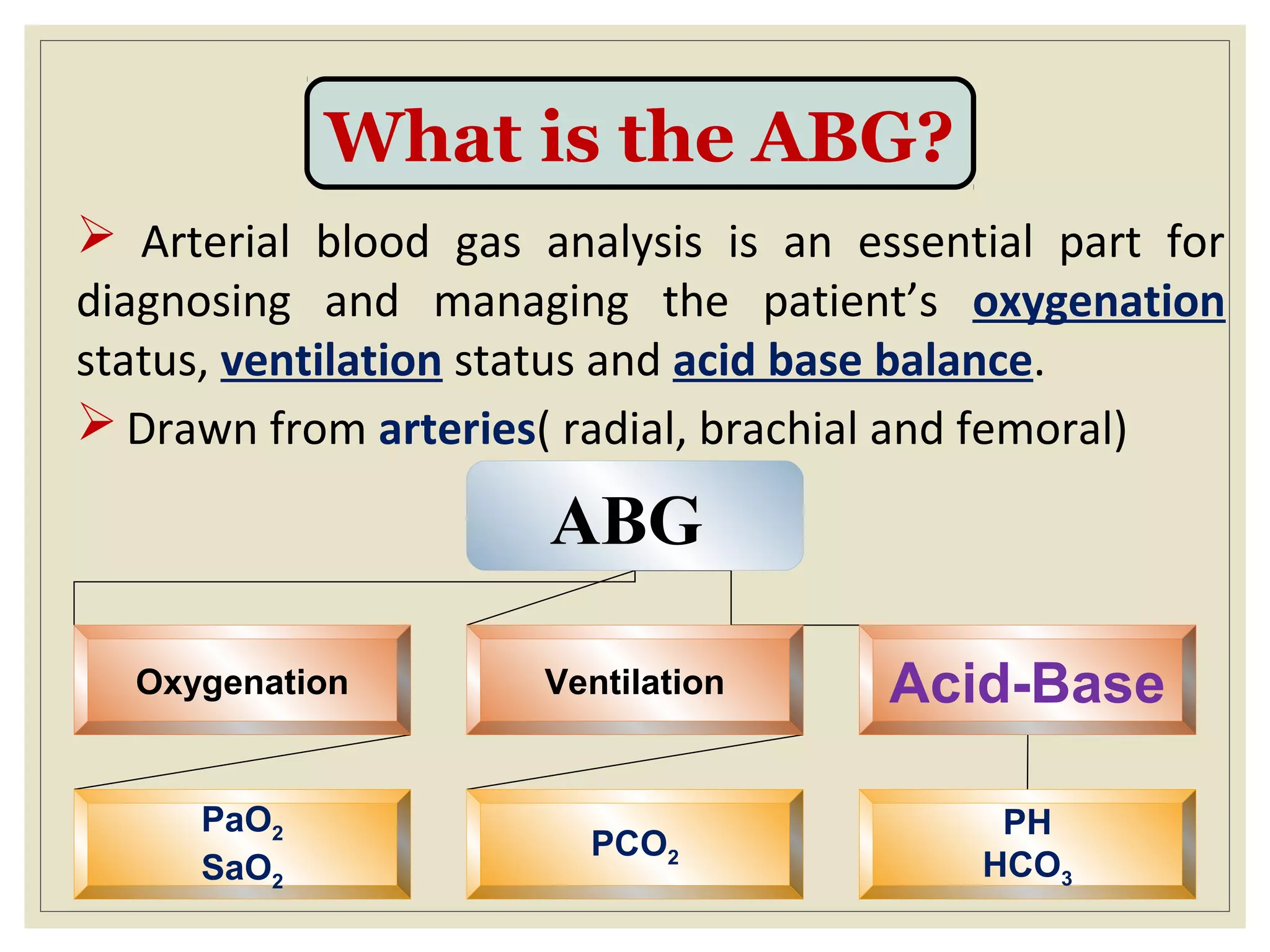
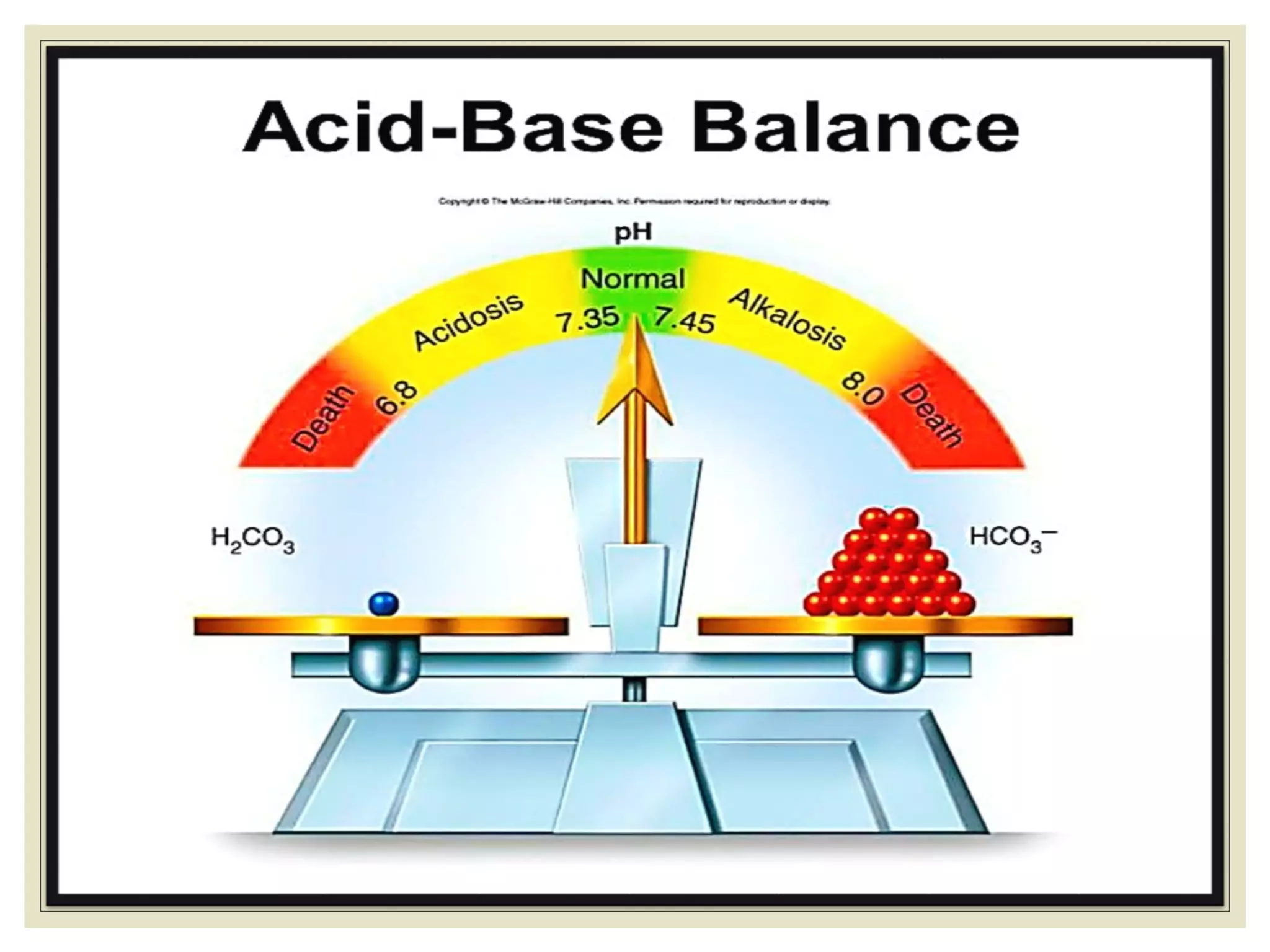
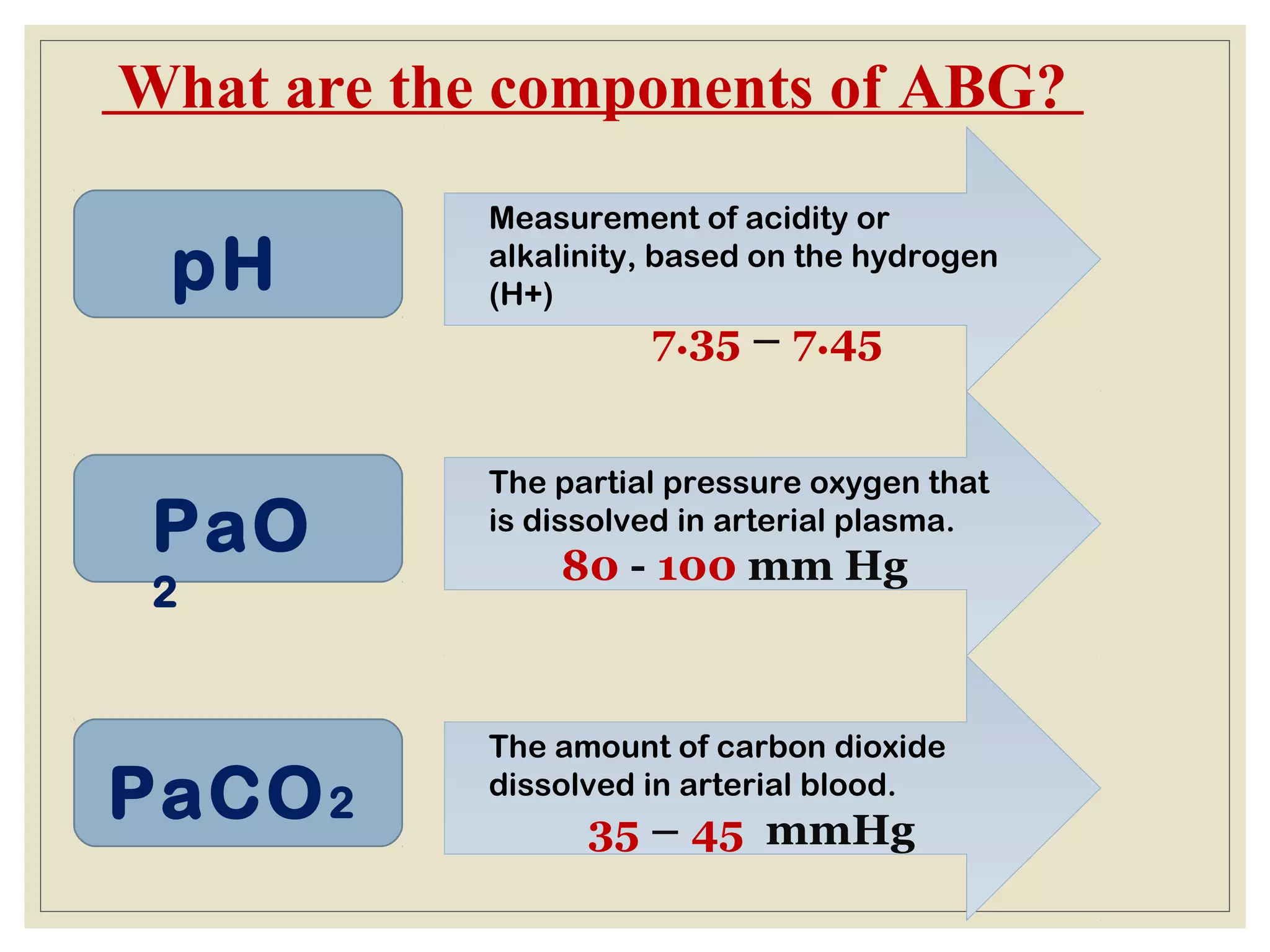
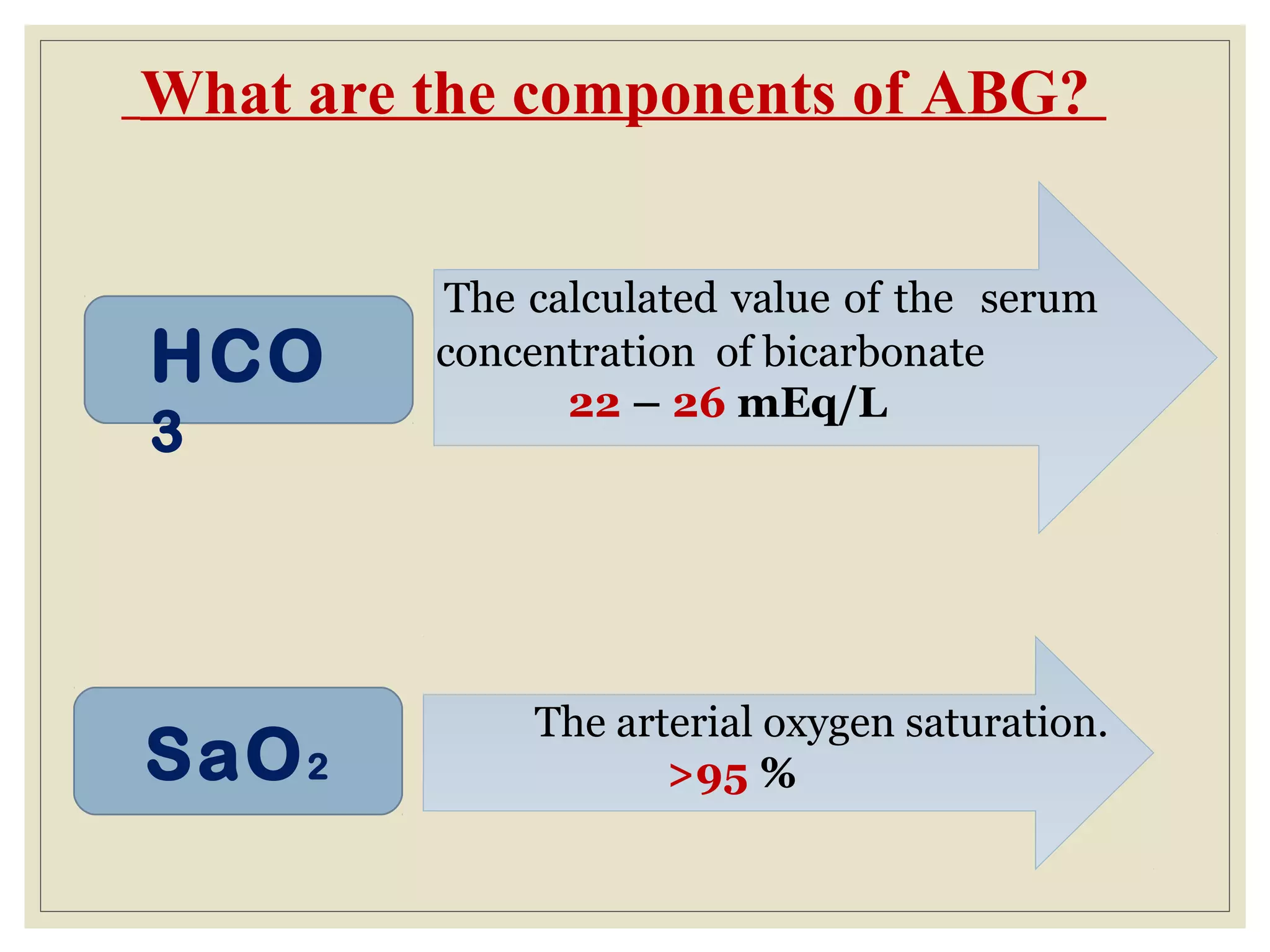
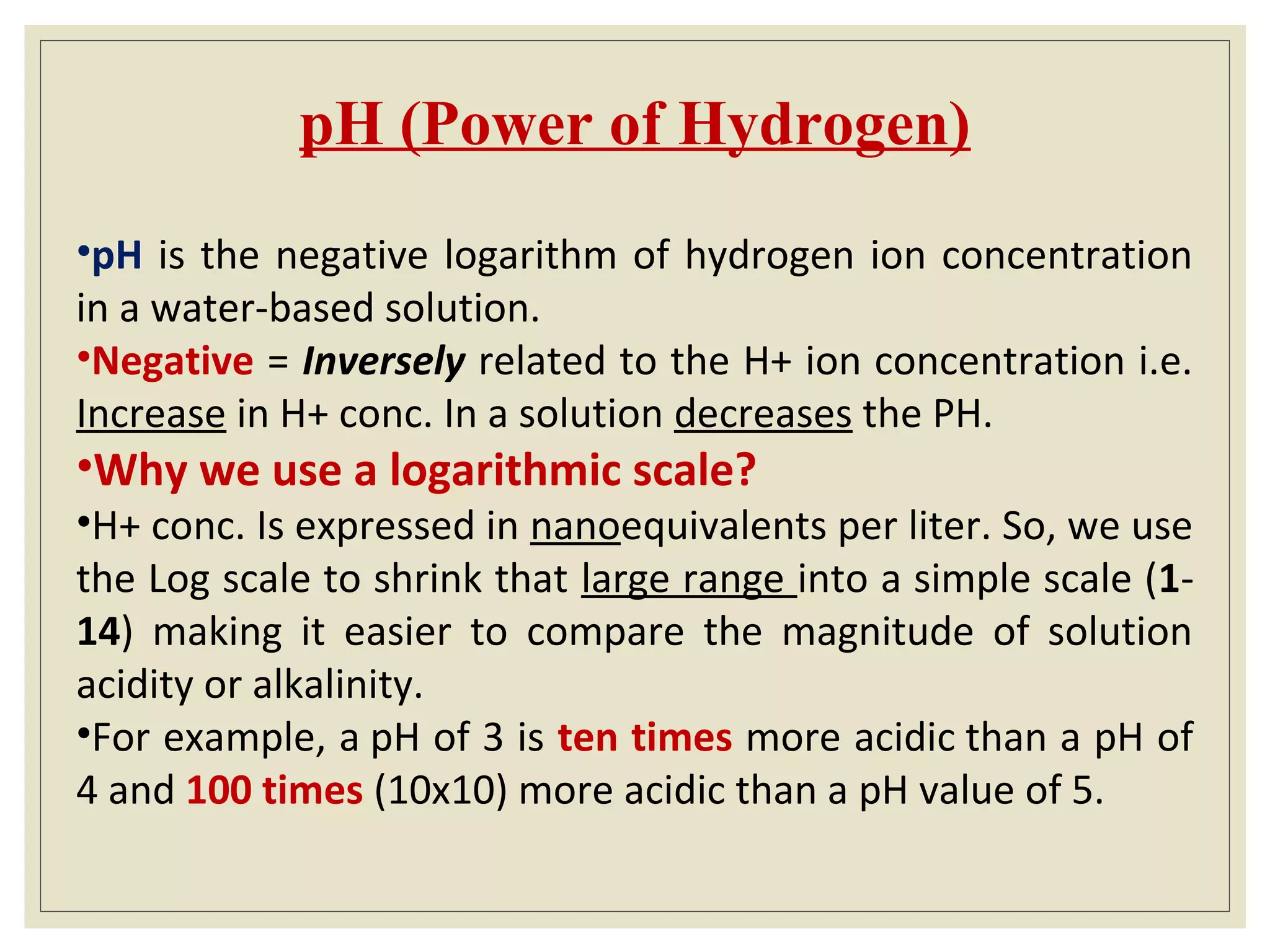
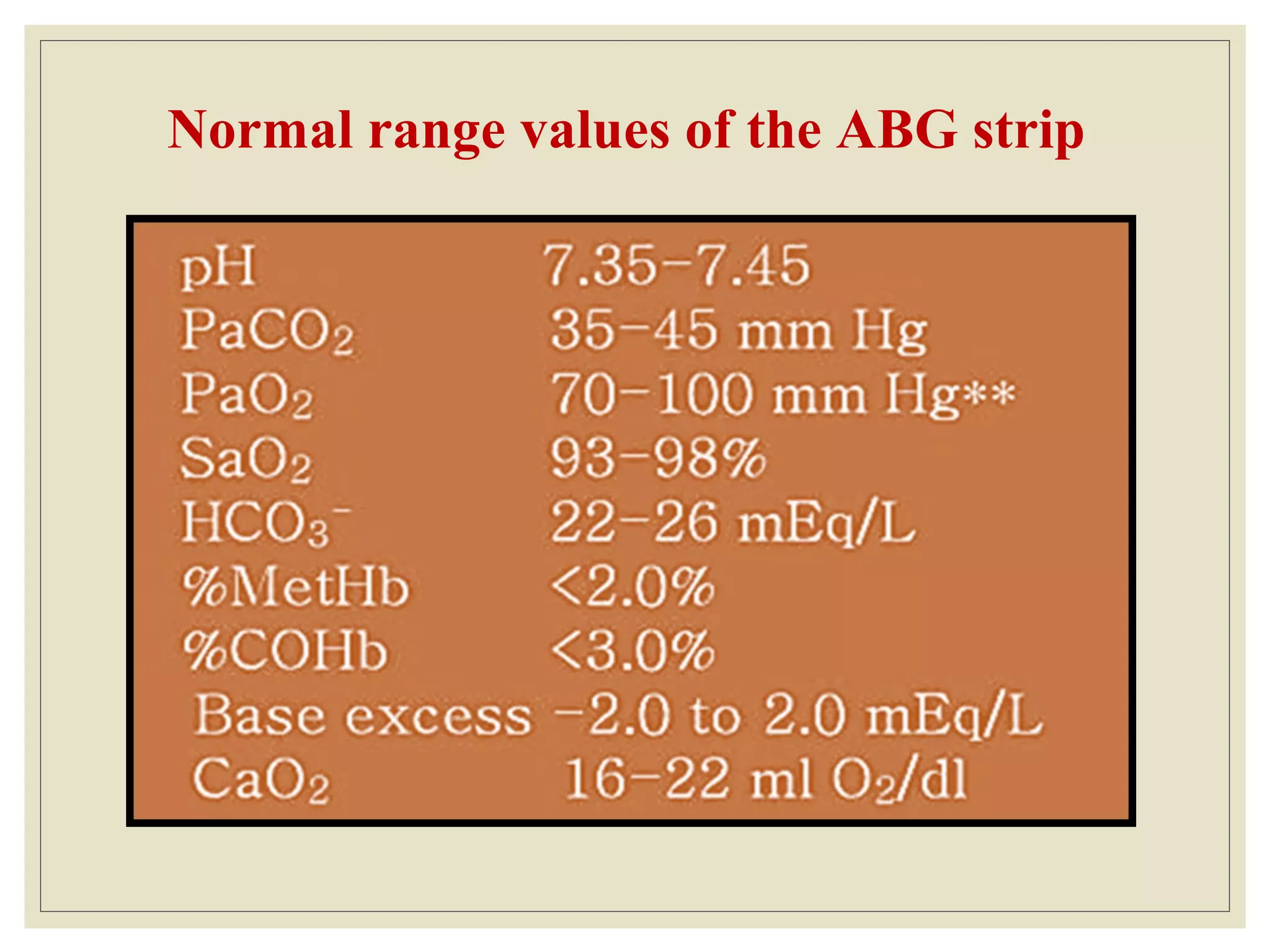
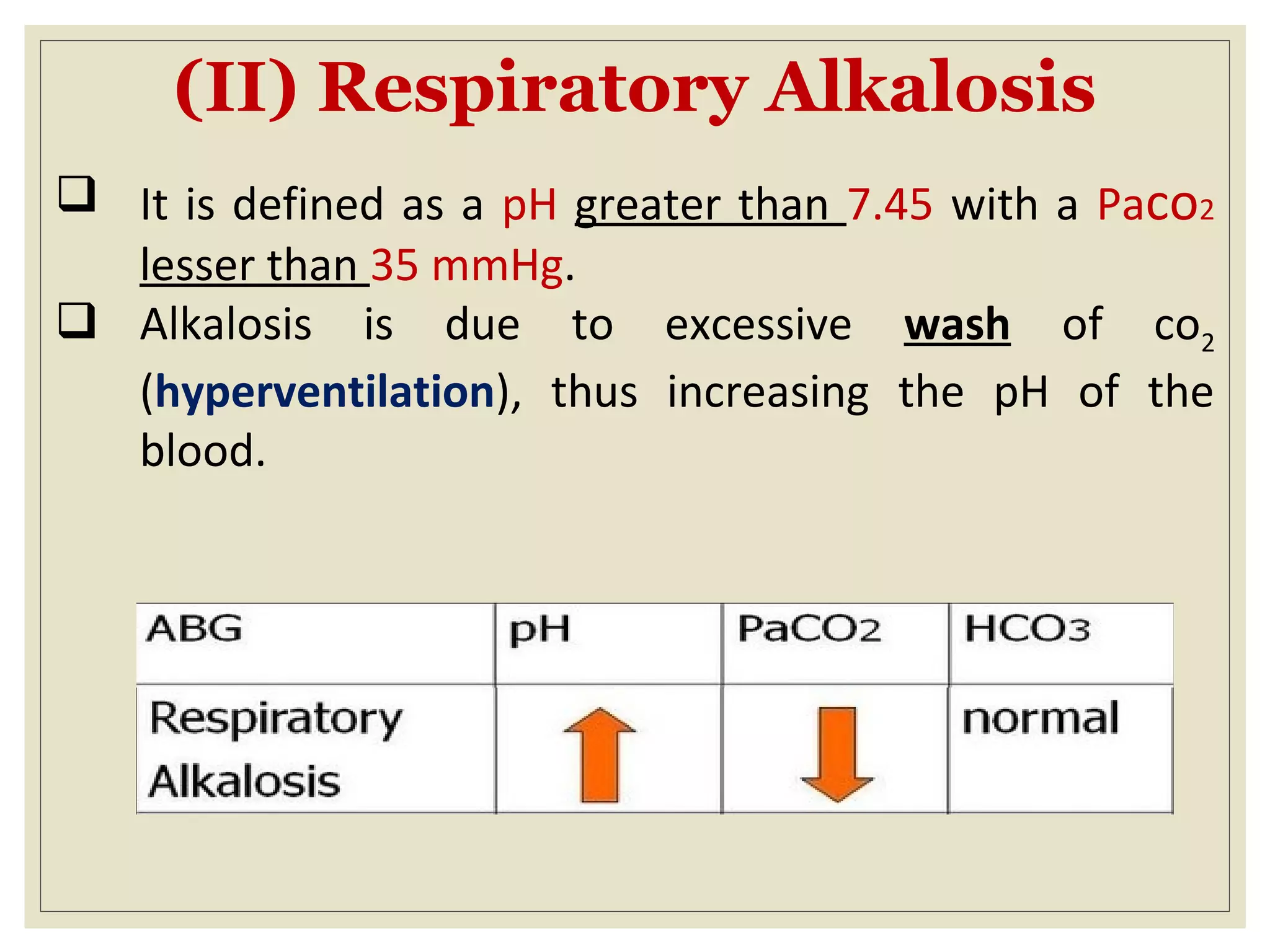
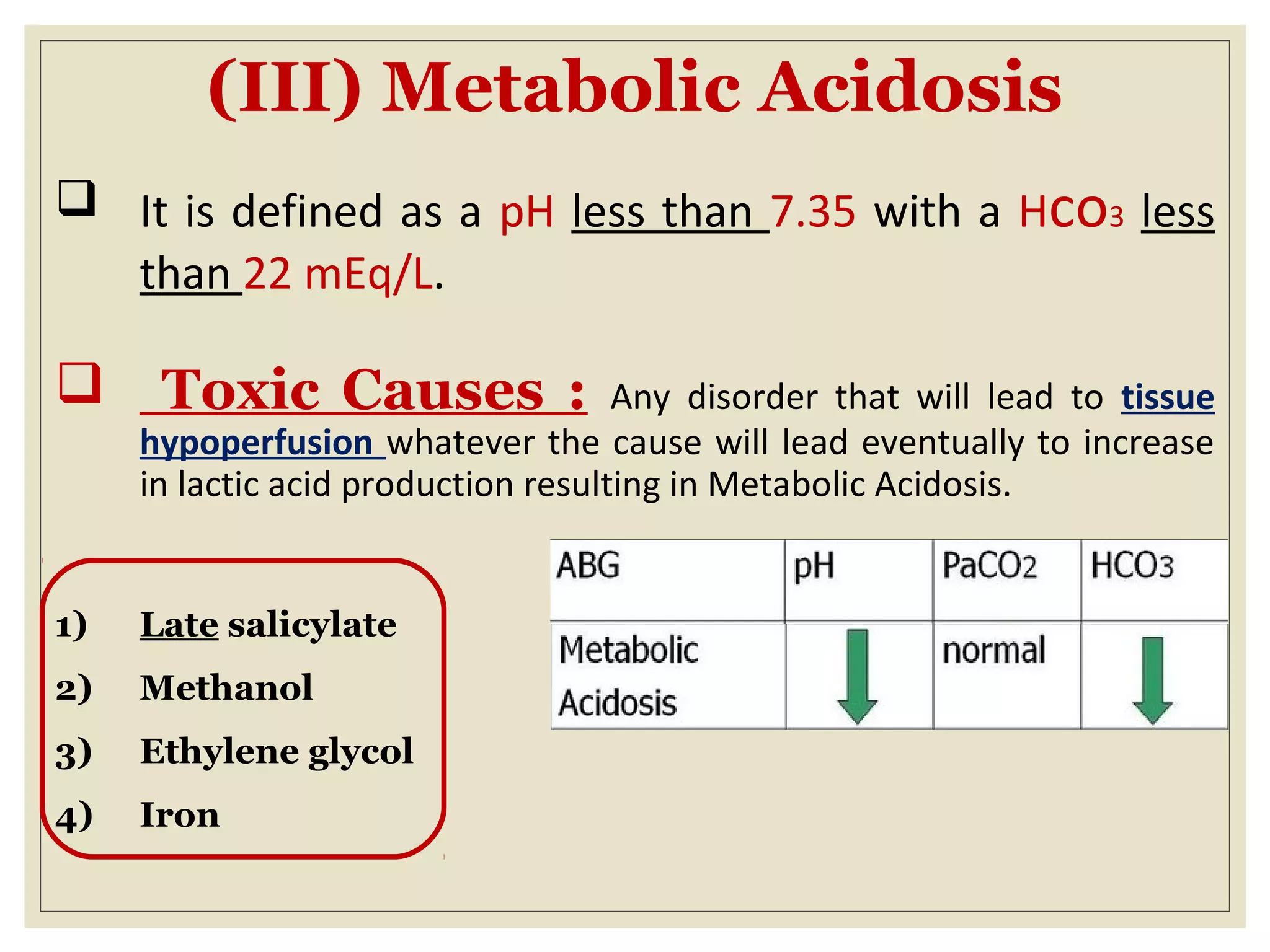
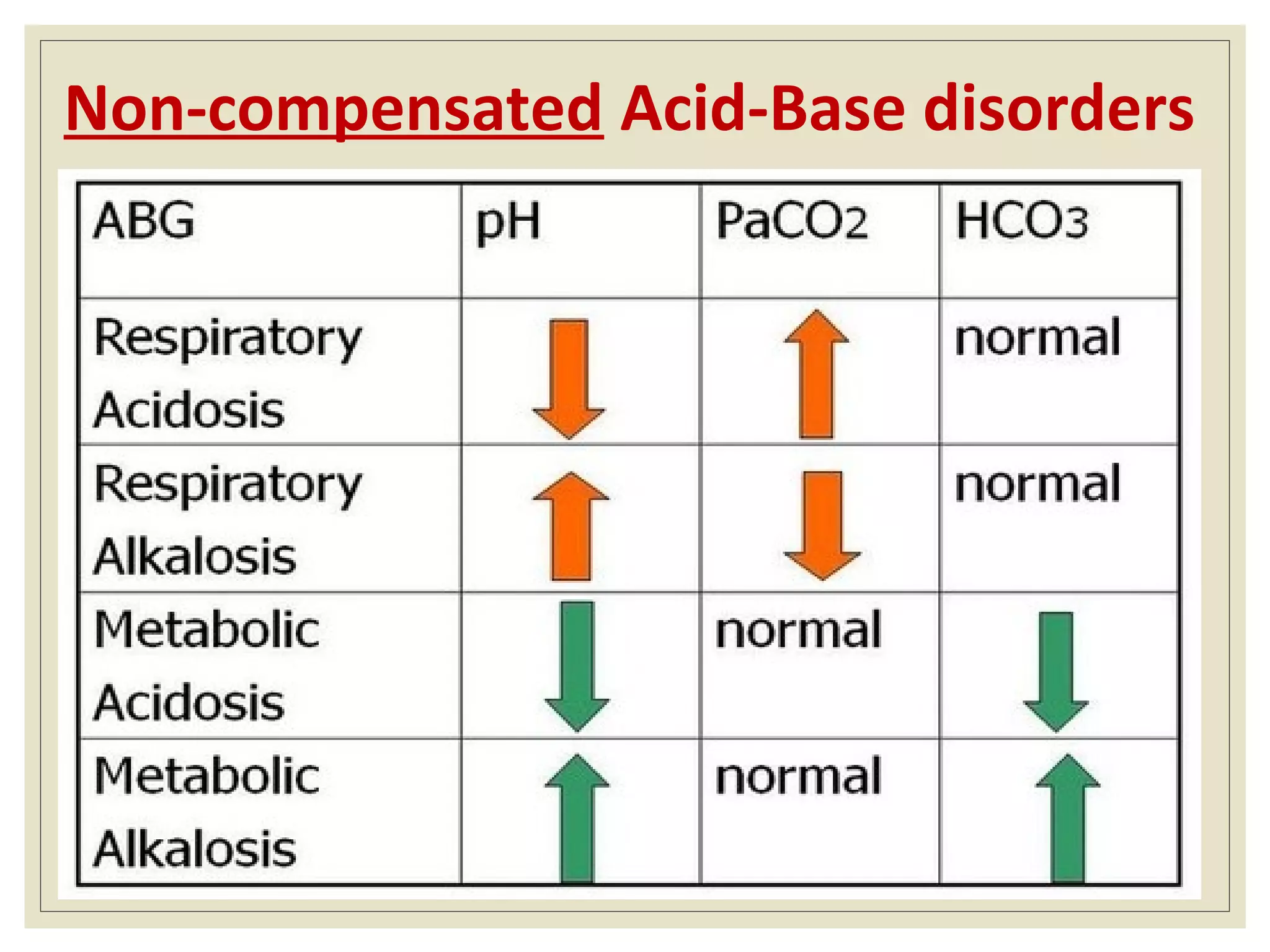
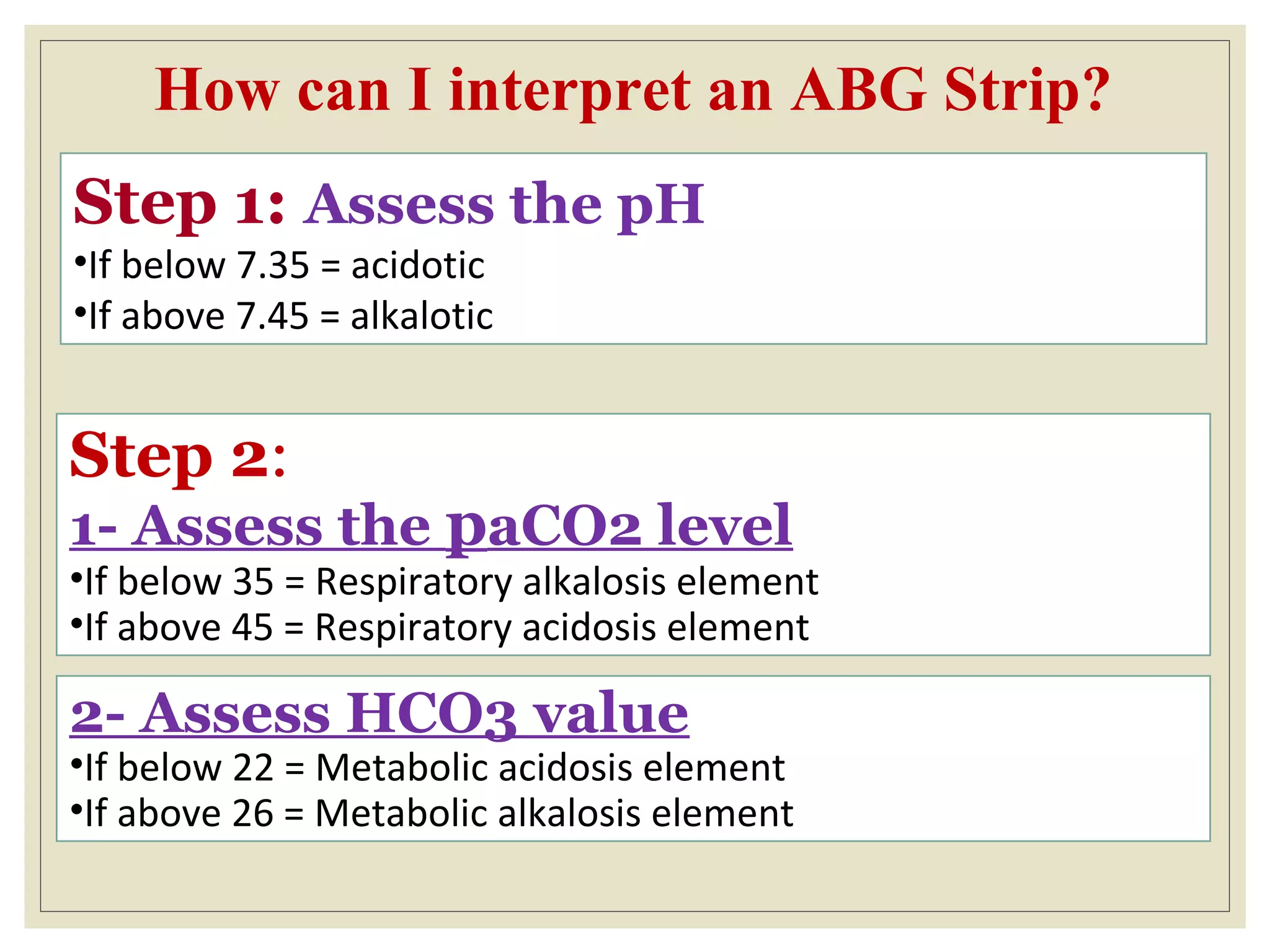
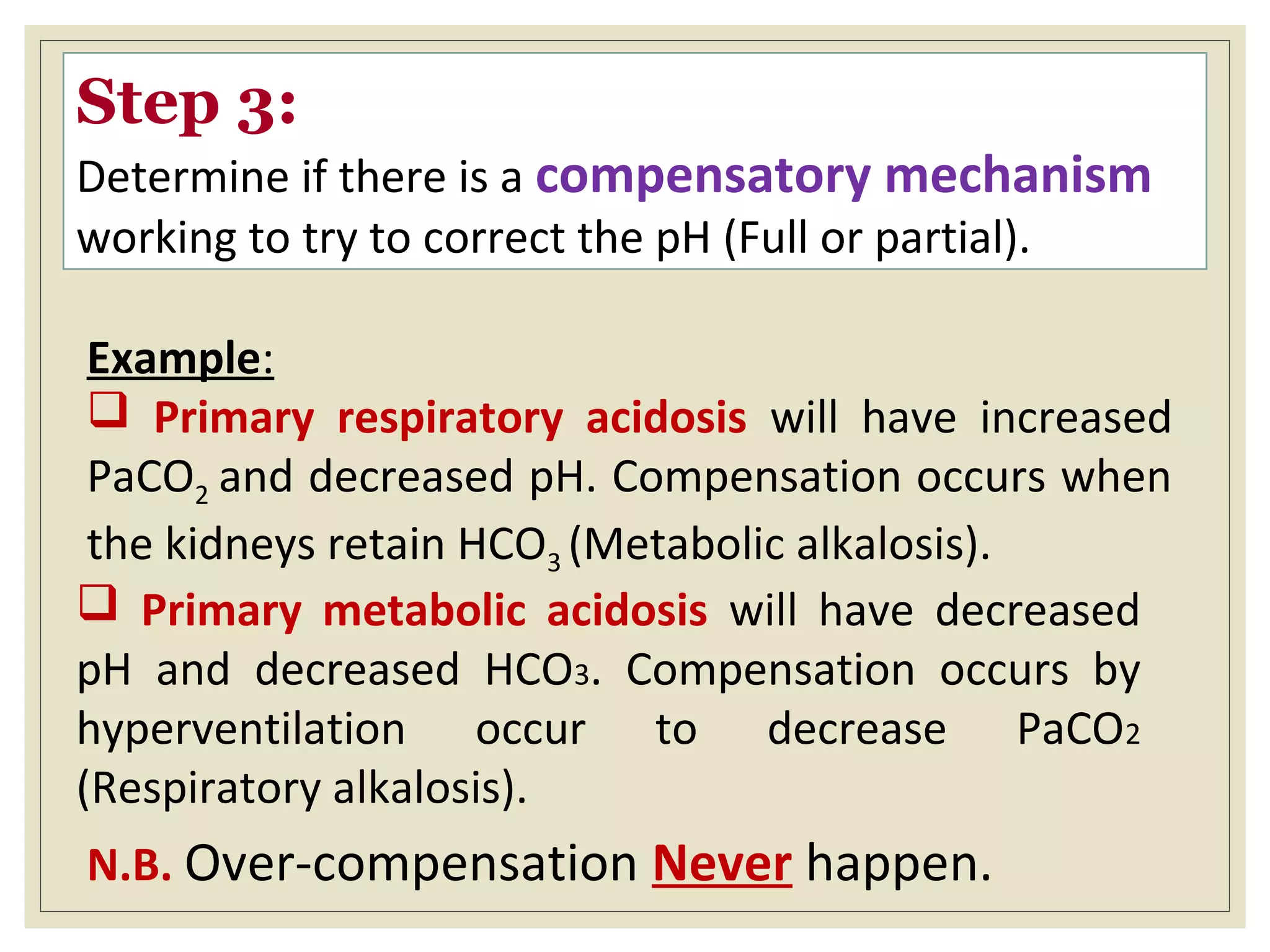
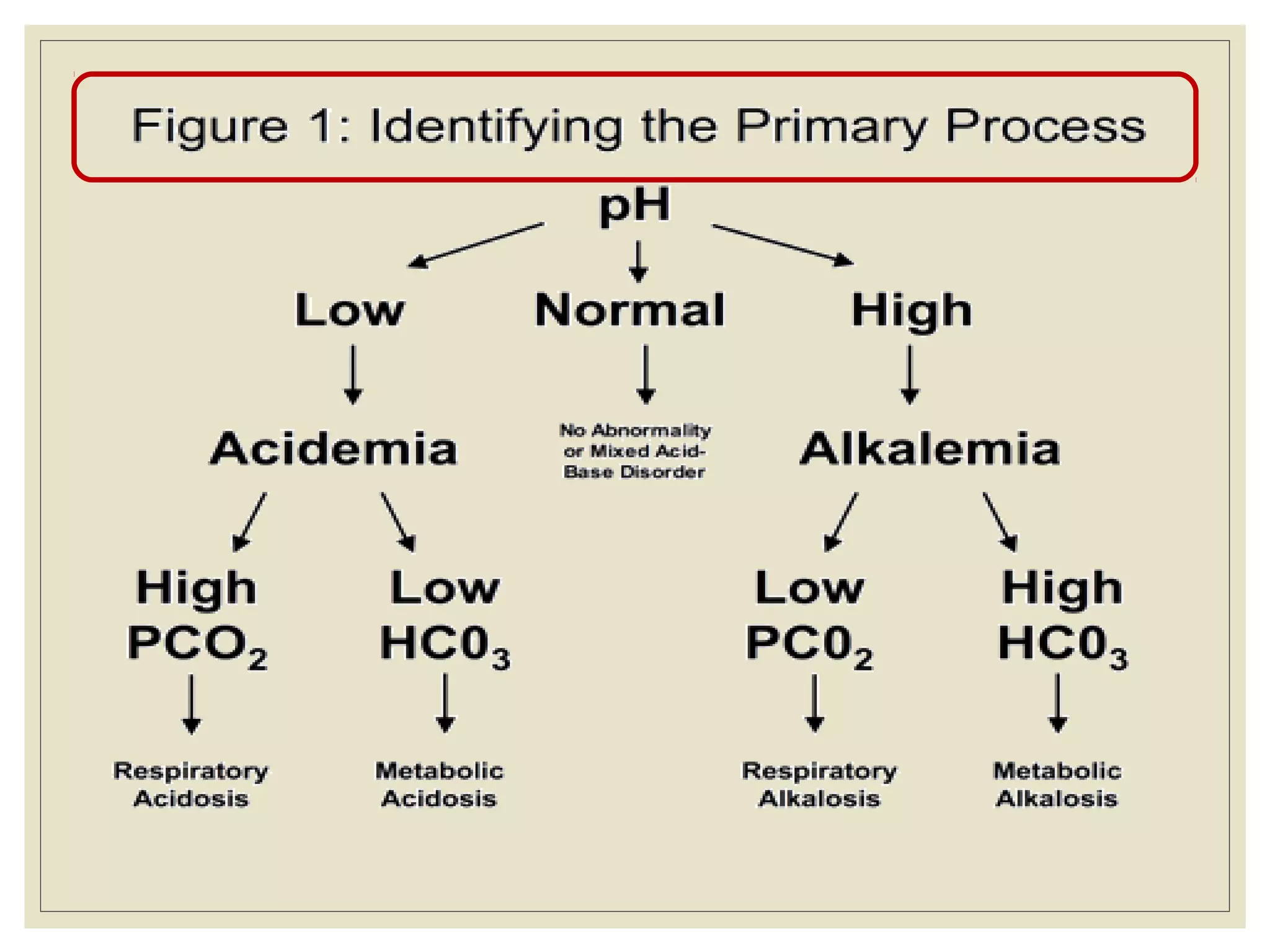
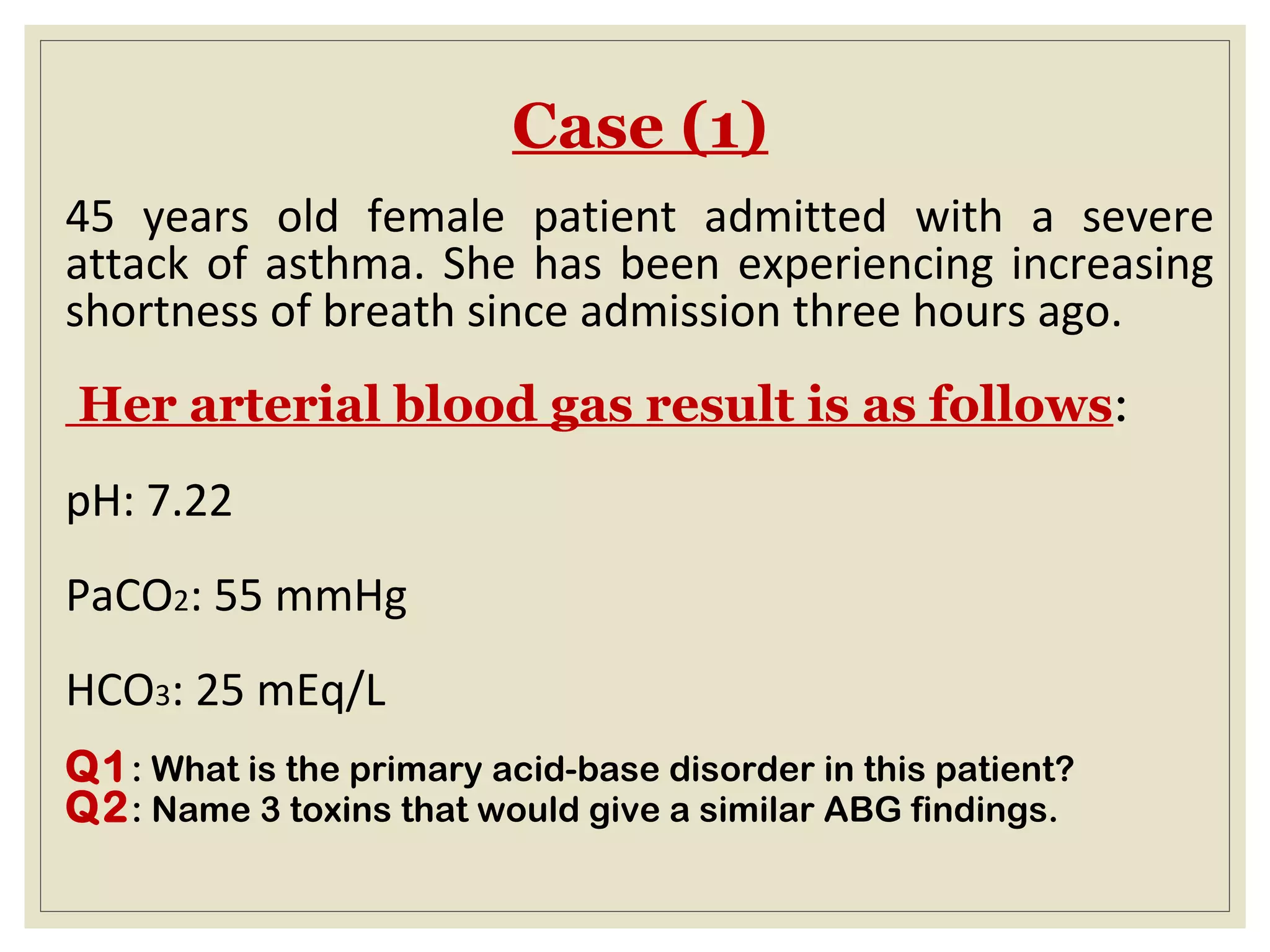
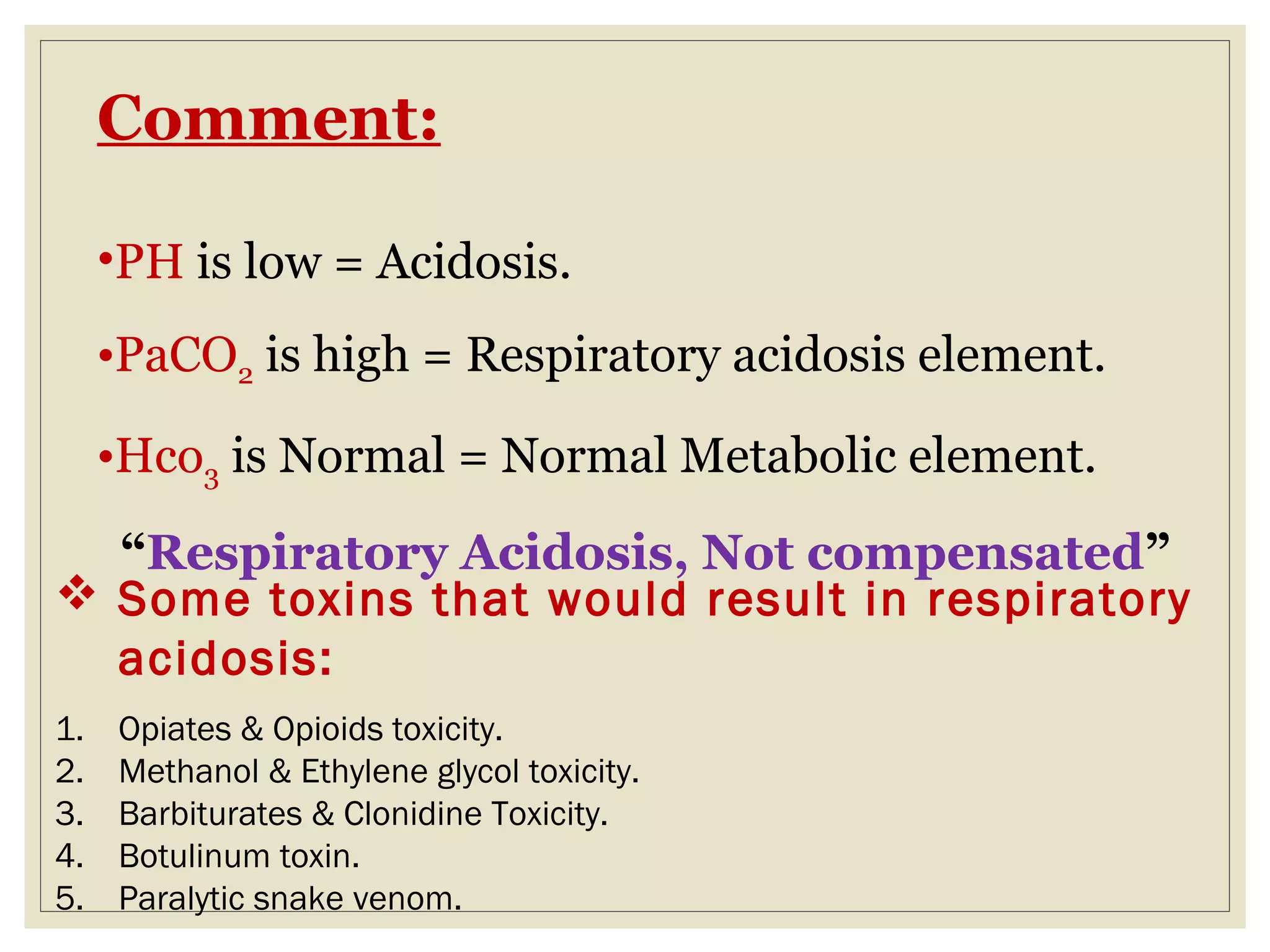
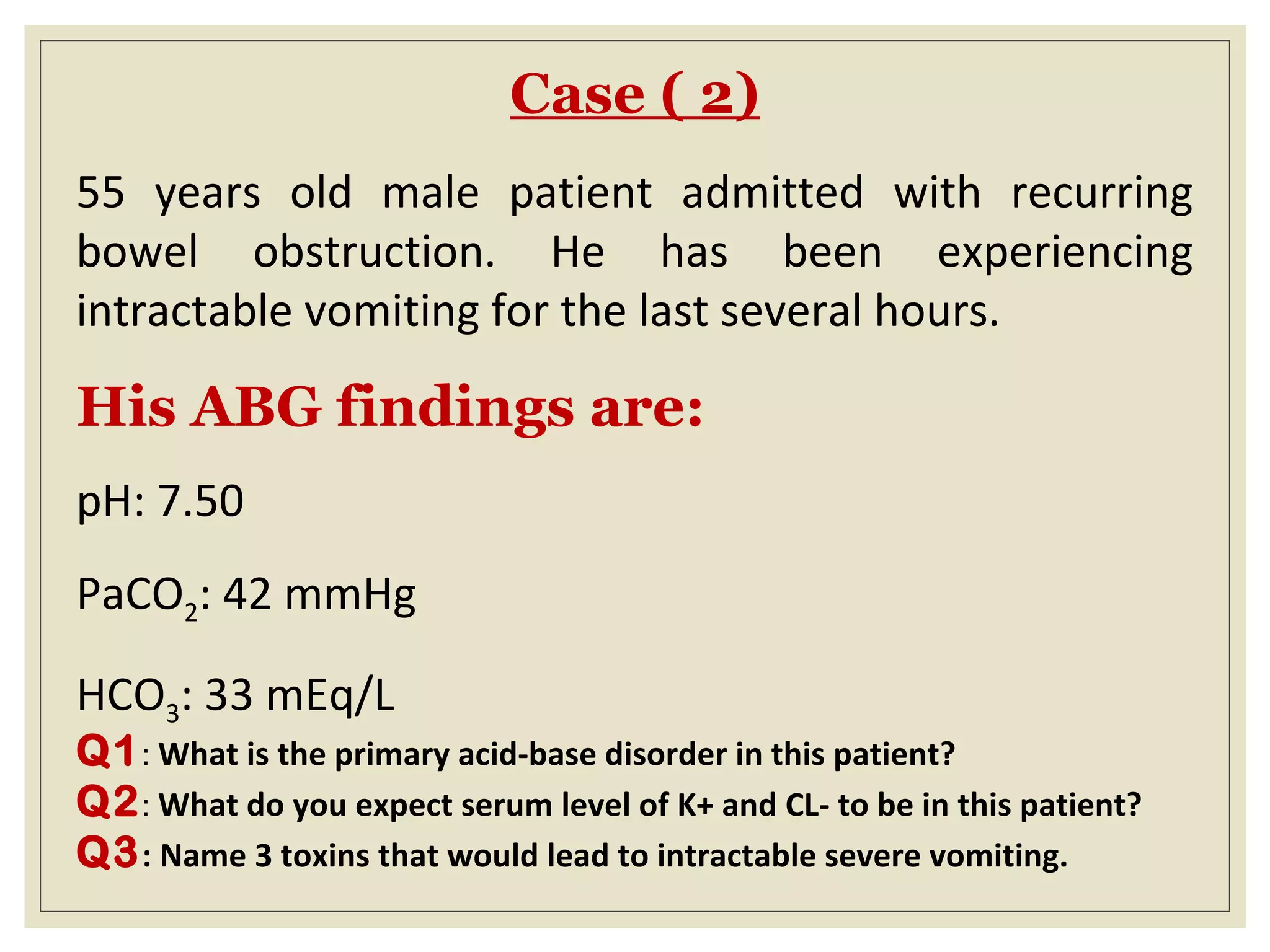
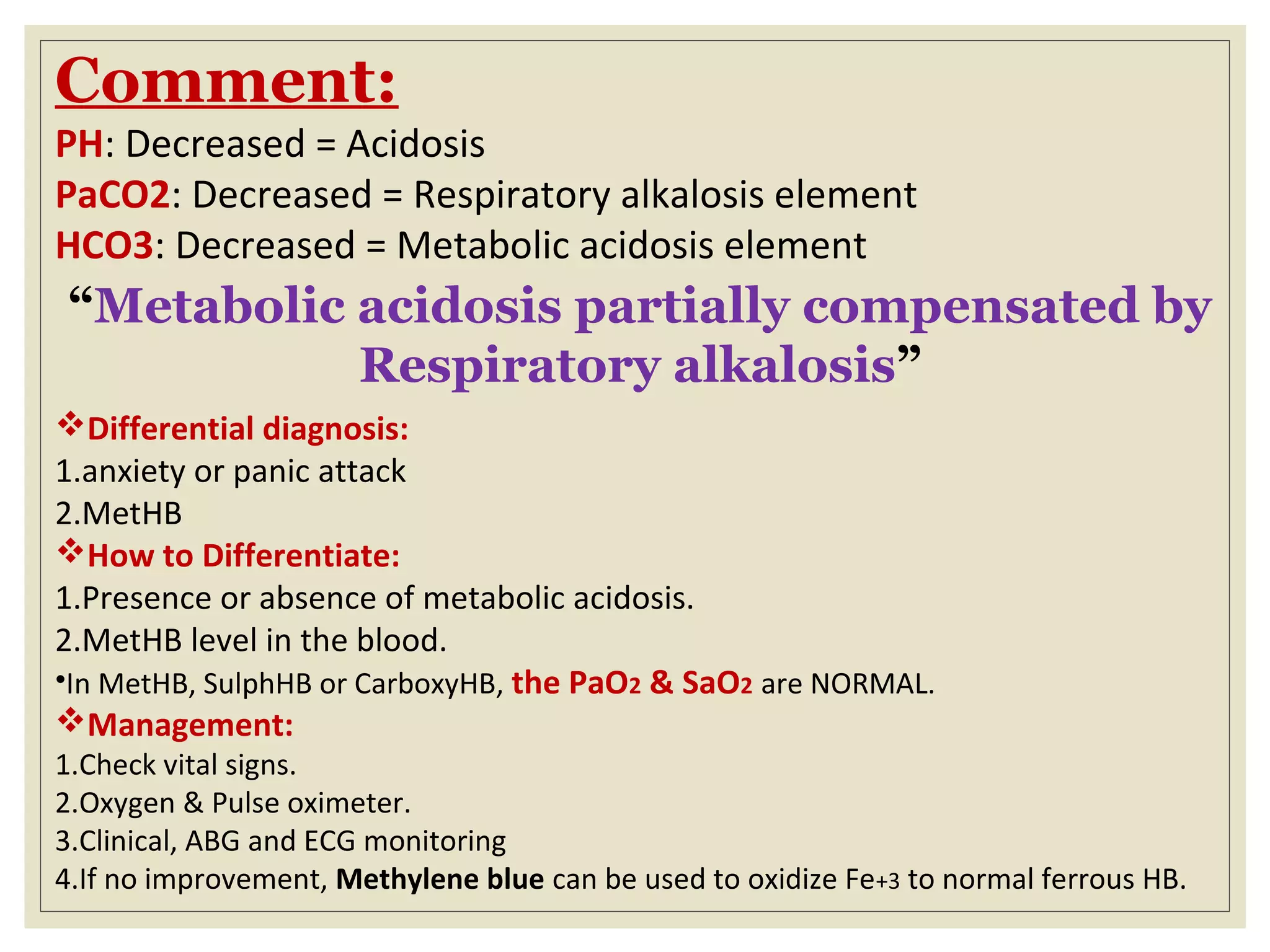


This document defines an arterial blood gas (ABG) analysis and its components. It discusses the normal acid-base balance and how acid-base imbalances present as respiratory or metabolic acidosis or alkalosis. Specific examples of each type of acid-base disorder are provided along with their typical causes, signs, symptoms, and management approaches. Common toxins that can cause acid-base disturbances are also listed. The document aims to equip readers to interpret ABG results in the clinical toxicology setting.

































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)








