Download to read offline
![Supervised Exercise, Stent Revascularization,
or Medical Therapy for Claudication
Due to Aortoiliac Peripheral Artery Disease
The CLEVER Study
[Claudication: Exercise Versus Endoluminal
Revascularization ]
JOURNAL OF THE AMERICAN COLLEGE OF
CARD IOLOGY
VOL. 65, NO. 10, 2015](https://image.slidesharecdn.com/supervisedexercisestentrevascularization-150511154636-lva1-app6892/85/Supervised-Exercise-Stent-Revascularization-or-Medical-Therapy-for-Claudication-Due-to-Aortoiliac-Peripheral-Artery-Disease-1-320.jpg)
![Supervised Exercise, Stent Revascularization,
or Medical Therapy for Claudication
Due to Aortoiliac Peripheral Artery Disease
The CLEVER Study
[Claudication: Exercise Versus Endoluminal
Revascularization ]
JOURNAL OF THE AMERICAN COLLEGE OF
CARD IOLOGY
VOL. 65, NO. 10, 2015](https://image.slidesharecdn.com/supervisedexercisestentrevascularization-150511154636-lva1-app6892/75/Supervised-Exercise-Stent-Revascularization-or-Medical-Therapy-for-Claudication-Due-to-Aortoiliac-Peripheral-Artery-Disease-1-2048.jpg)
![BACKGROUND
• Treatment for claudication that is due to
aortoiliac peripheral artery disease (PAD) often
relies on stent revascularization (ST).
• However, supervised exercise (SE) is known to
provide comparable short-term (6-month)
improvements in functional status and quality
of life. [Circulation. 2012 January 3]
• Longer-term outcomes are not known.](https://image.slidesharecdn.com/supervisedexercisestentrevascularization-150511154636-lva1-app6892/85/Supervised-Exercise-Stent-Revascularization-or-Medical-Therapy-for-Claudication-Due-to-Aortoiliac-Peripheral-Artery-Disease-2-320.jpg)
![• PAD is one of the most prevalent
cardiovascular diseases, affecting up to 5% of
individuals over 55 years of age.[Circulation
2004;110:738–43]
• Clinical trials have demonstrated that
supervised exercise (SE) is an effective
treatment because it significantly improves
walking performance.[JAMA 1995;274:975–
80], and quality of life. [J Vasc Surg 1996;
23:104–15]
• Despite this, access to SE is limited, because
clinicians do not actively prescribe this
claudication treatment.](https://image.slidesharecdn.com/supervisedexercisestentrevascularization-150511154636-lva1-app6892/85/Supervised-Exercise-Stent-Revascularization-or-Medical-Therapy-for-Claudication-Due-to-Aortoiliac-Peripheral-Artery-Disease-3-320.jpg)



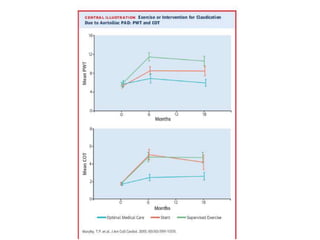

This randomized controlled trial compared supervised exercise (SE), stent revascularization (ST), and optimal medical care (OMC) in patients with claudication due to aortoiliac peripheral artery disease. At 6 months, SE resulted in better treadmill walking performance than ST, but ST led to better patient-reported quality of life. At 18 months, treadmill walking improved most for SE, more for ST, and least for OMC, while quality of life gains were similar for SE and ST and less for OMC. The study concludes that SE provides durable and comparable benefits to ST for up to a year after completion of supervised training.



































![Webinar_3_Exercise_in_PAD_slides[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/webinar3exerciseinpadslides1-230108171846-c03927af-thumbnail.jpg?width=640&height=640&fit=bounds)

















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



