This document provides an overview of peripheral neuropathy, including:
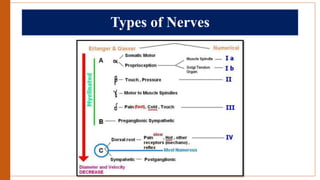
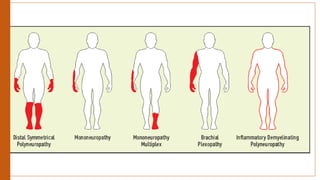
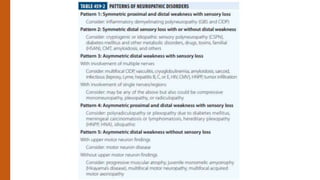
- Types of peripheral neuropathy are classified based on whether they primarily affect motor nerves, sensory nerves, or both.
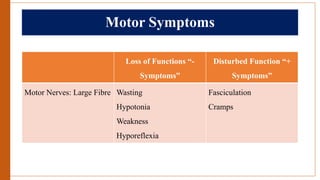
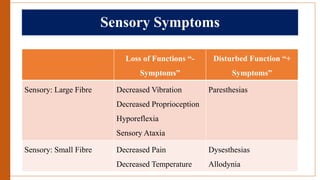
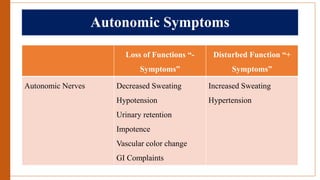
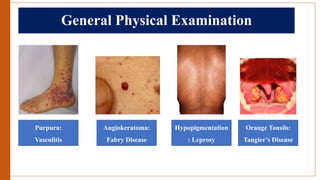
- The main symptoms of motor, sensory, and autonomic neuropathies are described.
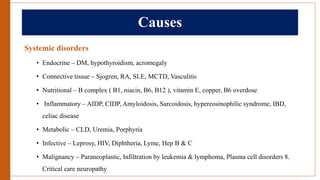
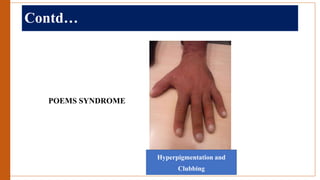
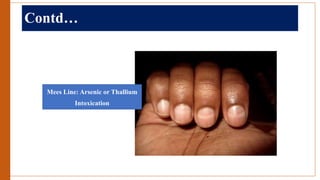
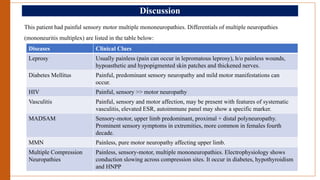
- The most common causes of peripheral neuropathy include systemic disorders like diabetes, connective tissue diseases, nutritional deficiencies, infections, malignancies and toxic neuropathies.
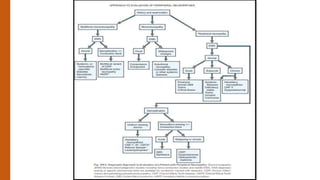
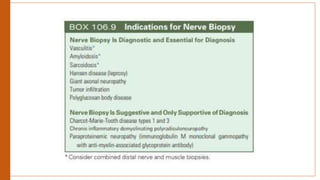
- The approach to evaluating a patient with peripheral neuropathy involves obtaining a history, neurological exam, electrodiagnostic studies and sometimes nerve biopsy to identify the location and cause of the neuropathy.




























































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















