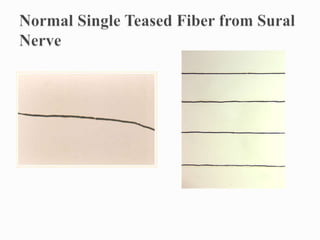
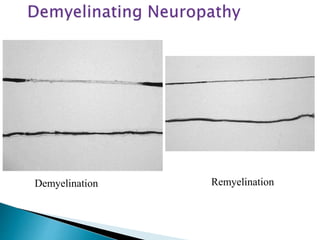
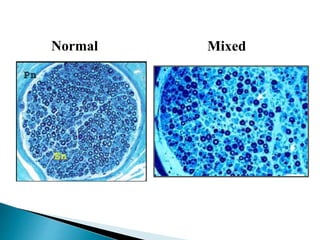
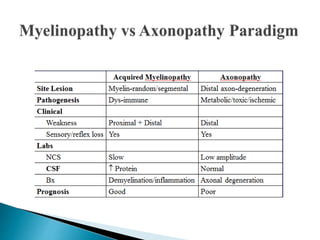
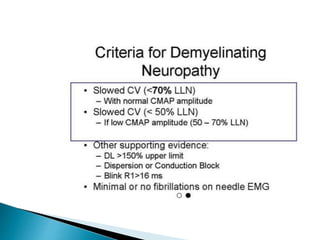
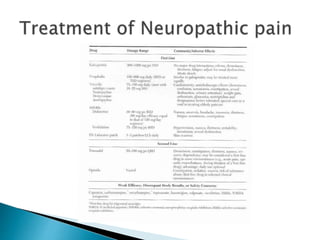
The document outlines an approach to peripheral neuropathy by discussing three main goals: determining the lesion location and pathology, identifying the cause of the lesion, and determining if there is a specific treatment or best management approach. It then reviews different patterns of neuropathies including myelinopathies, axonopathies, demyelination, remyelination, and discusses key questions to consider in the evaluation of peripheral neuropathies.
































































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)





























