This document discusses the approach to evaluating and managing palpitations. It defines palpitations and describes how to characterize them based on features like intermittent/sustained, regular/irregular, heart rate, onset/offset. Potential etiologies are arranged cardiac causes like arrhythmias or structural issues, extracardiac causes, and psychiatric causes. Evaluation involves history, exam, ECG, monitoring. Management depends on underlying rhythm or cause, and may include beta blockers, treatment of precipitants, or ablation for sustained arrhythmias.









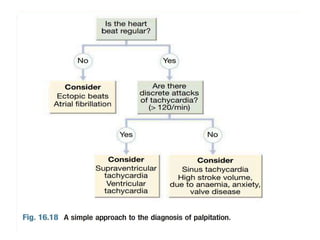








![Approach to palpitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/approachtopalpitationautosaved-170805225202-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































