Downloaded 30 times







![• Cell and tissue culture solutions like
Hbss
Saliva
Bovine milk and its variation
Green tea
Egg white
Coconut water
Braz Dent J. 2013 Sep-Oct;24(5):437-45]](https://image.slidesharecdn.com/pdl-190727162911/85/Periodontal-ligament-PDL-80-320.jpg)





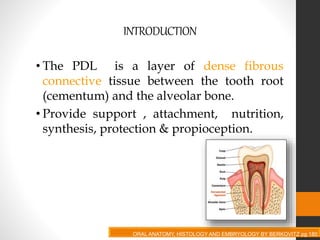
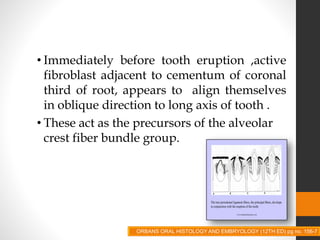
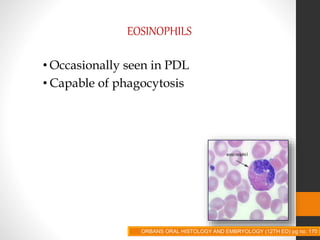
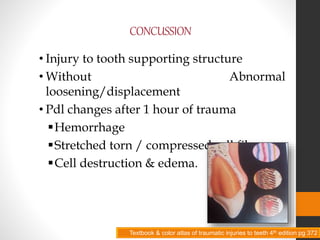
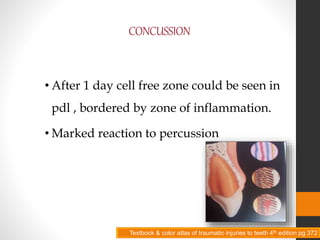
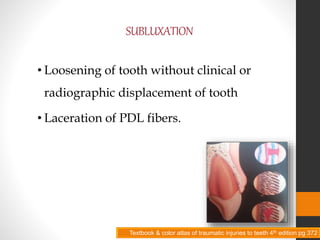
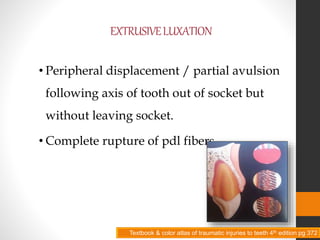
The document provides an in-depth overview of the periodontal ligament (PDL), covering its structure, development, histology, and clinical considerations. It discusses the PDL's functions, including support, attachment, and nutrition, as well as the various cellular components and fiber types within it. Additionally, the text addresses pathological conditions related to the PDL and the implications of trauma on its integrity.





















































































