Downloaded 317 times
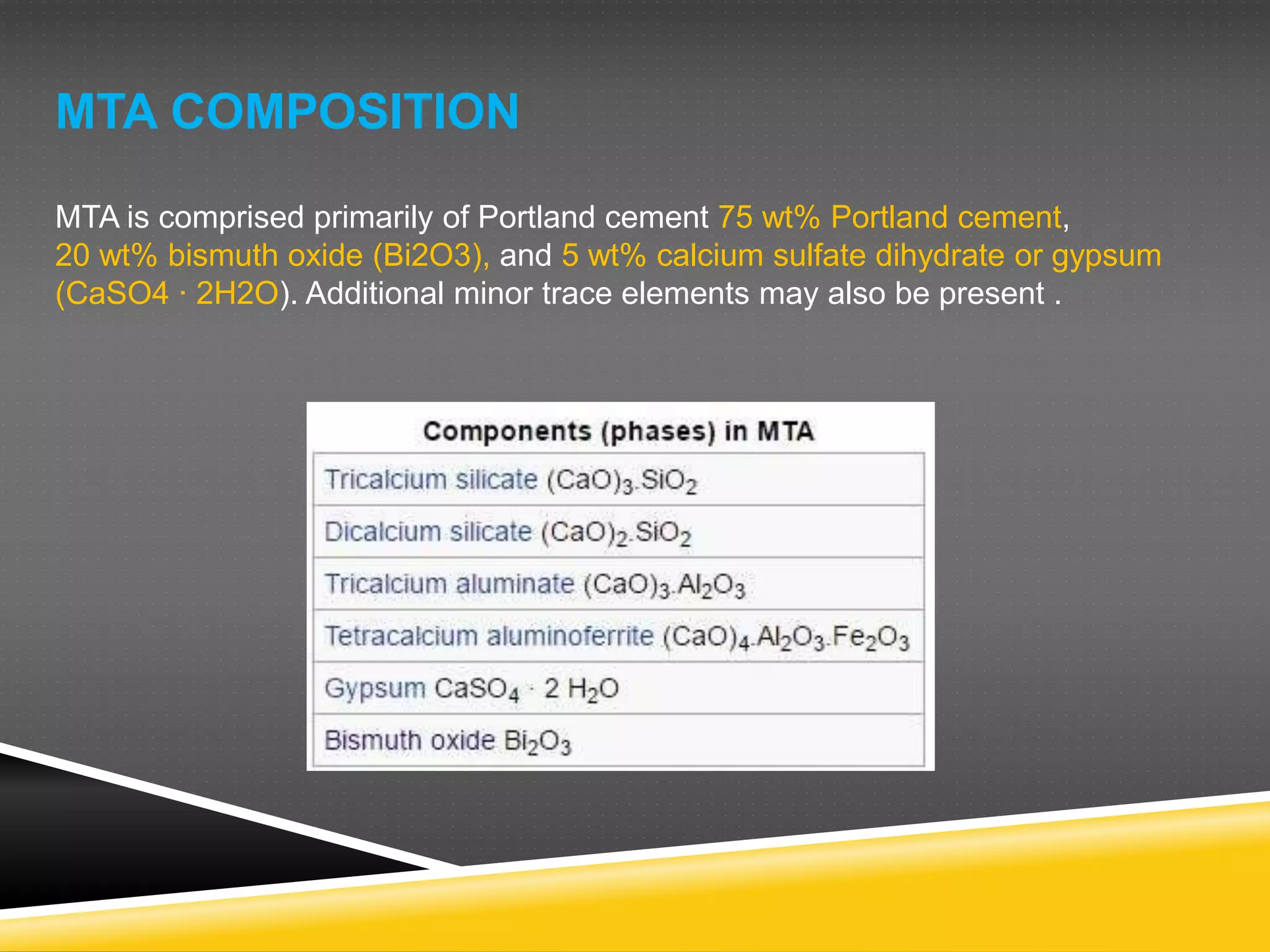
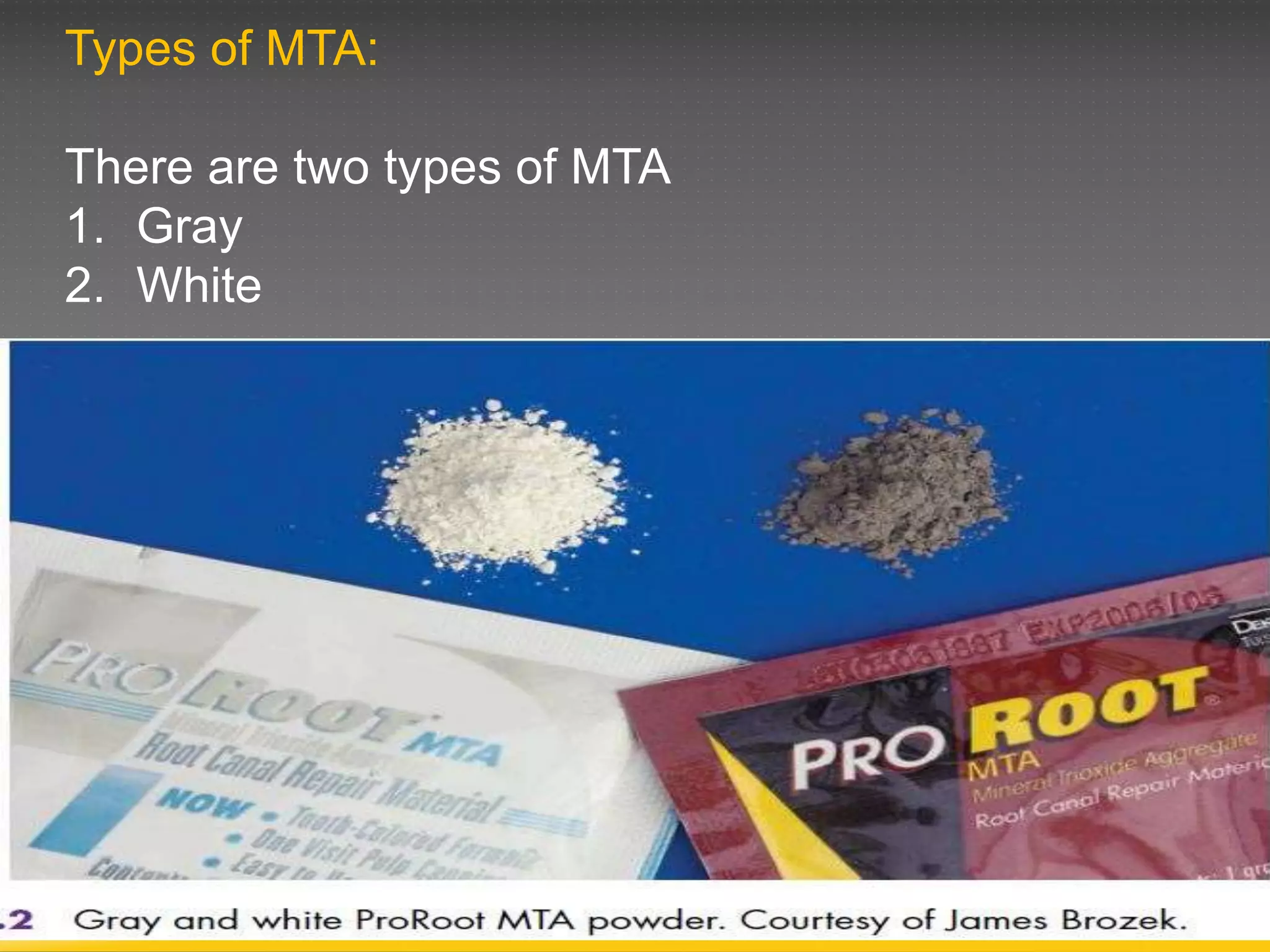
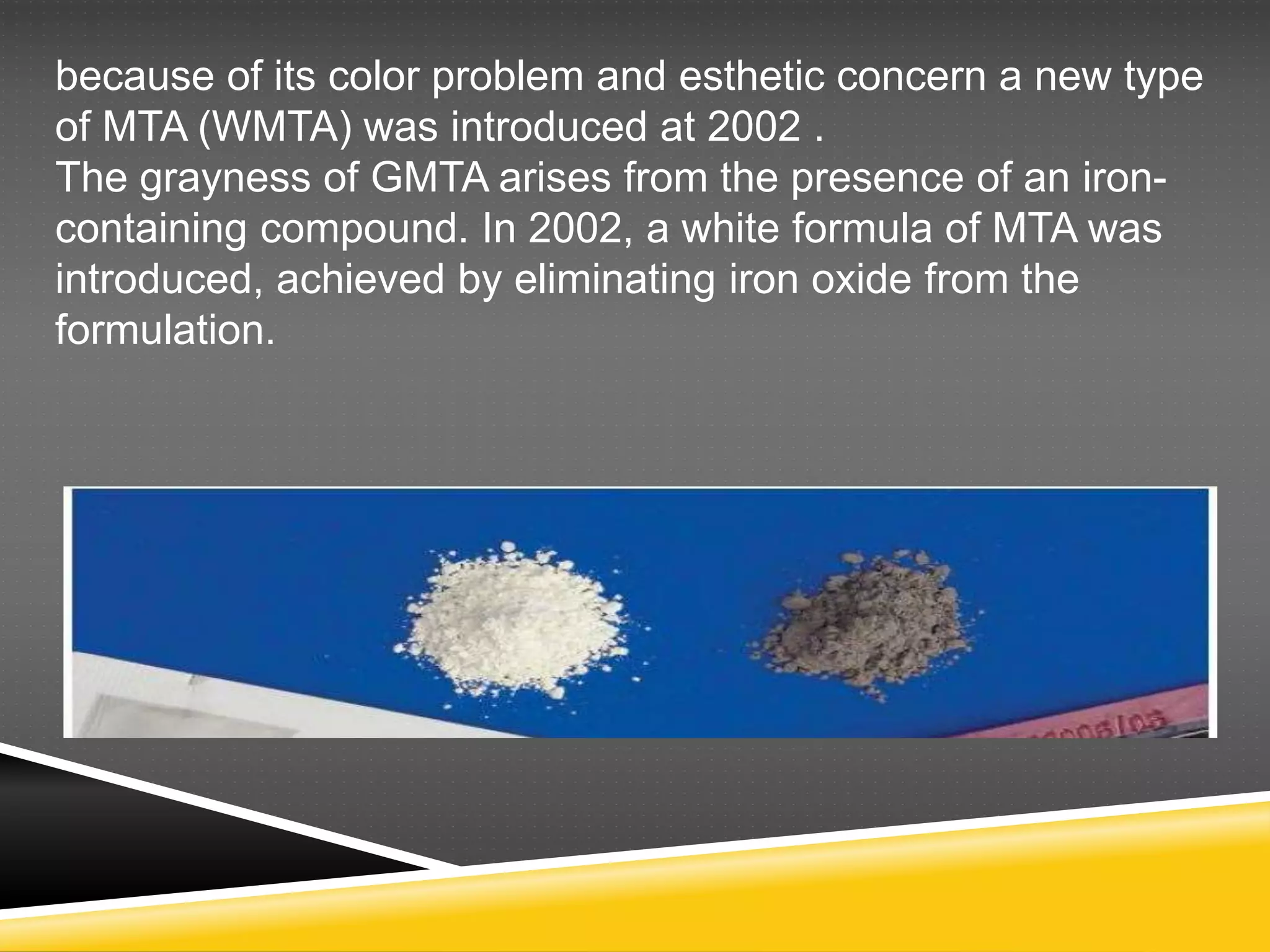
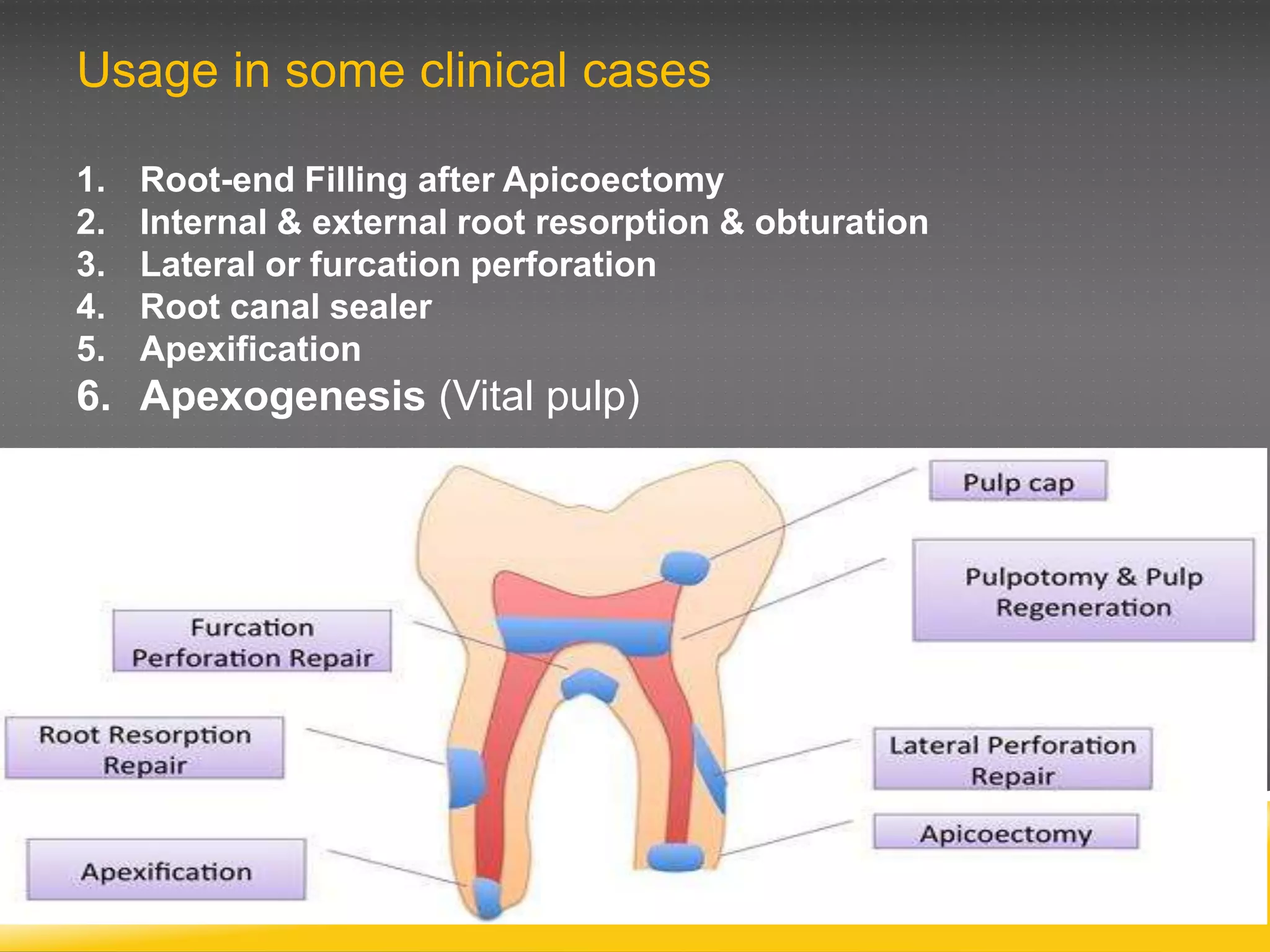



MTA was developed as a dental repair material and is composed primarily of Portland cement, bismuth oxide, and calcium sulfate. There are two types, gray and white. MTA is biocompatible, alkaline, and promotes hard tissue formation. It has applications in root-end fillings, perforation repairs, apexification, and pulp capping. Some disadvantages include long setting time and difficulty in manipulation.










































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












