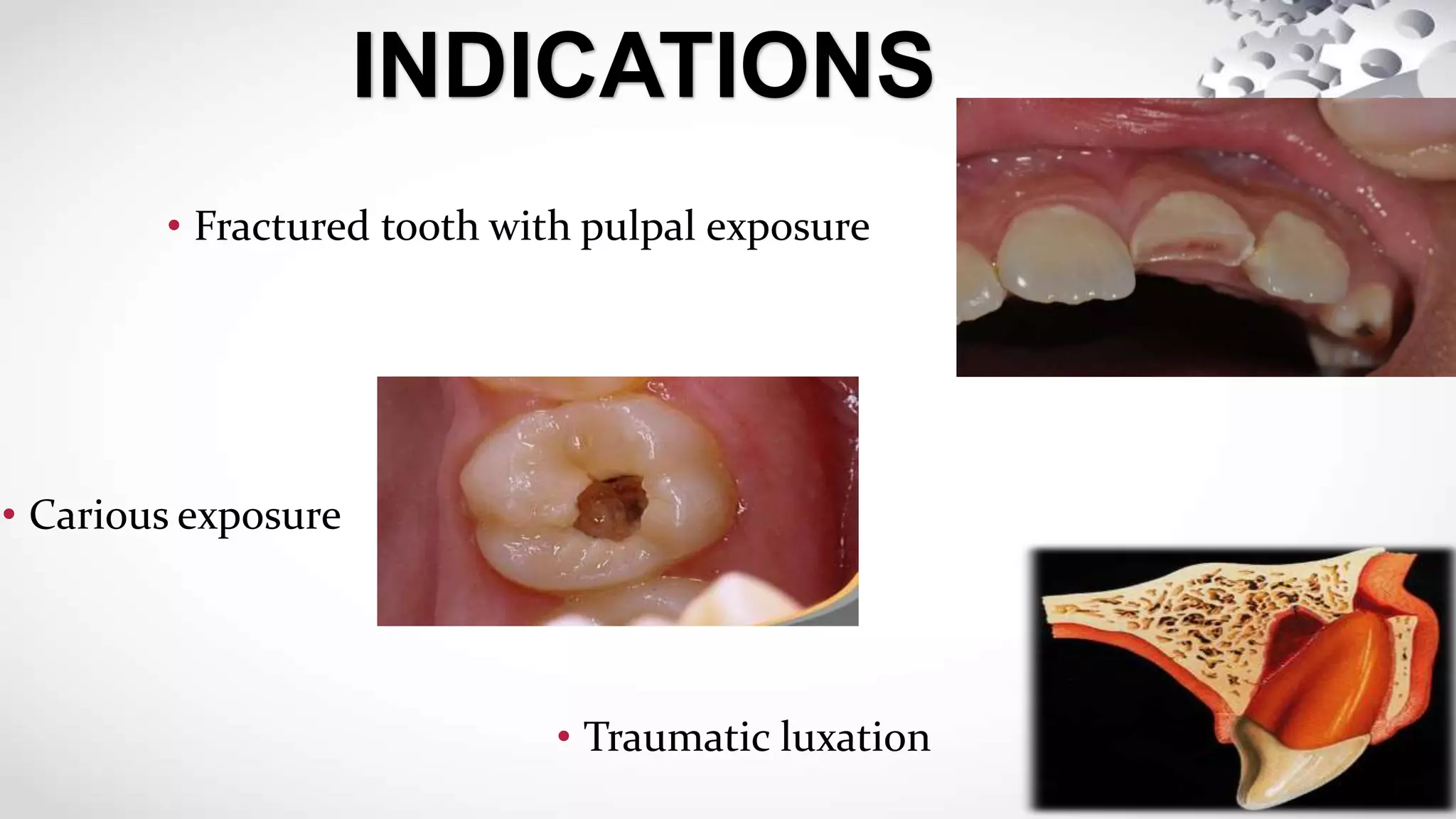
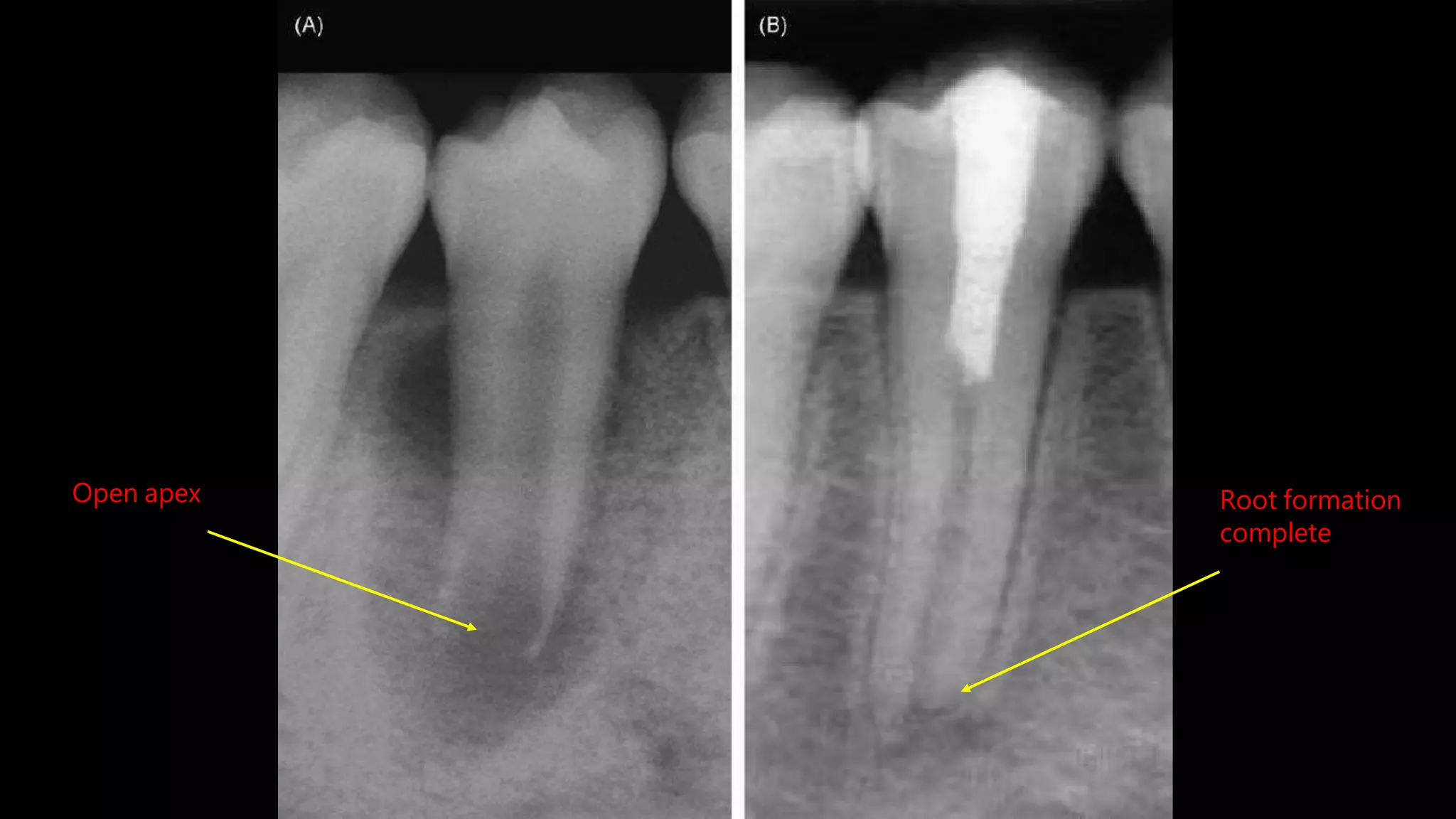
Apexogenesis involves pulp therapy procedures for immature permanent teeth with open apices to encourage continued root development. It aims to maintain pulp vitality and stimulate further root development and maturation. The procedures include indirect/direct pulp capping and pulpotomy, using materials like MTA or calcium hydroxide to cover the exposed pulp and encourage dentin bridge formation. Success is monitored by periodic radiographs to check for ongoing root formation and absence of pathology over several years.