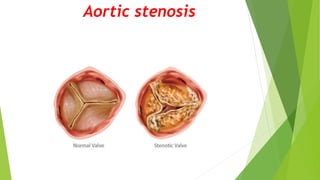
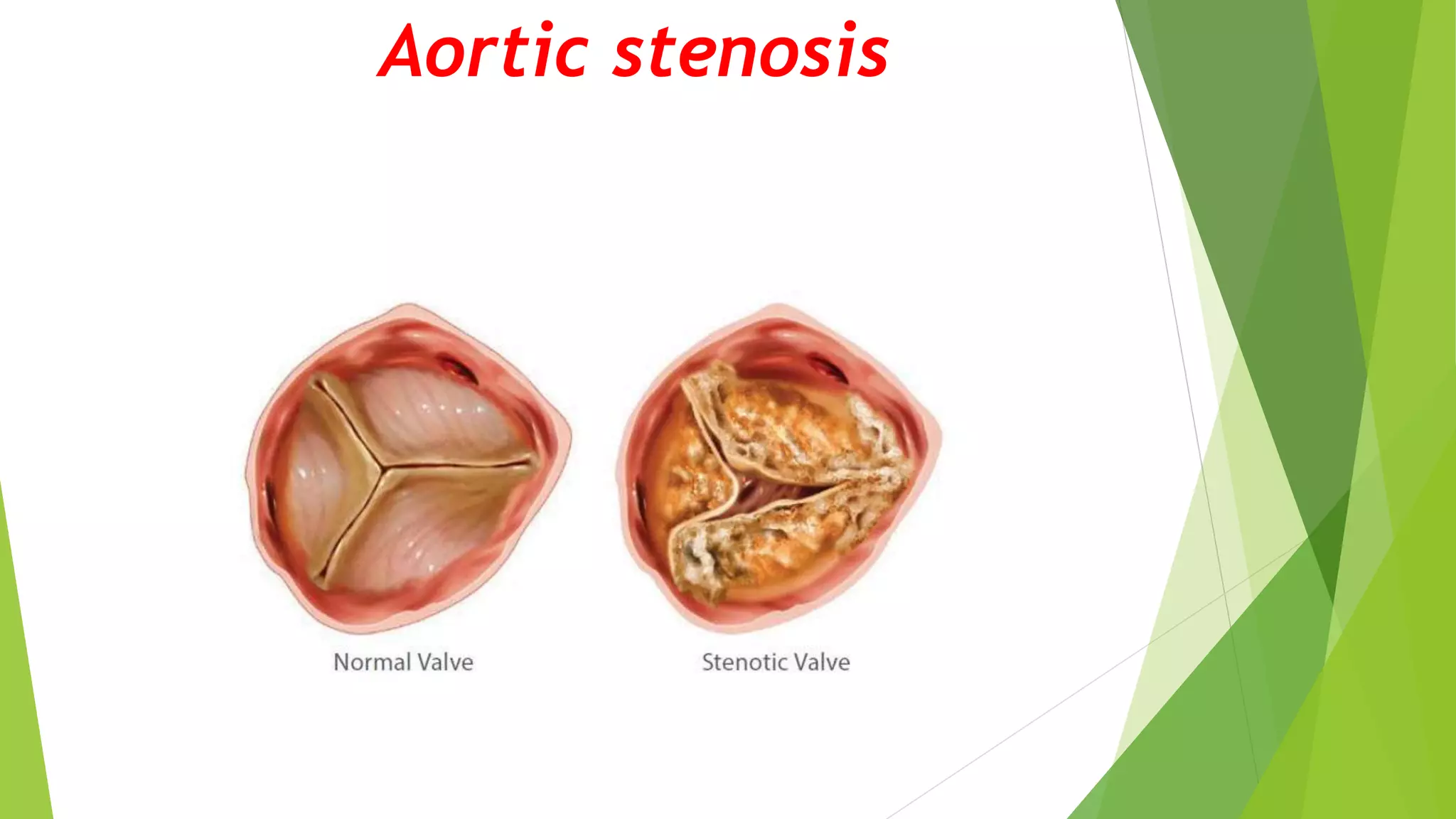
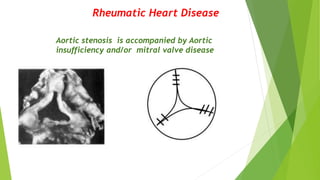
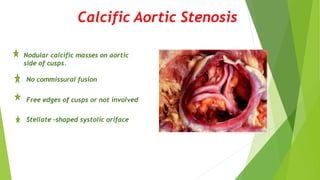
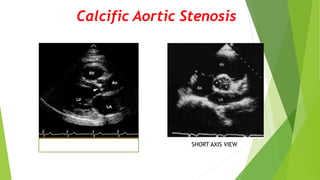
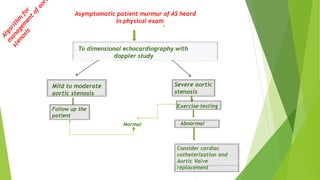
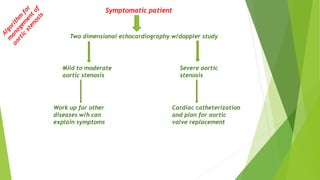
Aortic stenosis is a narrowing of the aortic valve opening that obstructs blood flow from the heart into the aorta. It has several causes including a congenitally abnormal bicuspid aortic valve, age-related degeneration and calcification of the valves, or rheumatic heart disease. Diagnosis involves echocardiography to measure the severity based on aortic valve area and pressure gradients. Severe aortic stenosis carries a poor prognosis without intervention, with 50% mortality within 3 years of symptom onset. Treatment options include surgical aortic valve replacement or the minimally invasive transcatheter aortic valve replacement procedure.