Downloaded 19 times

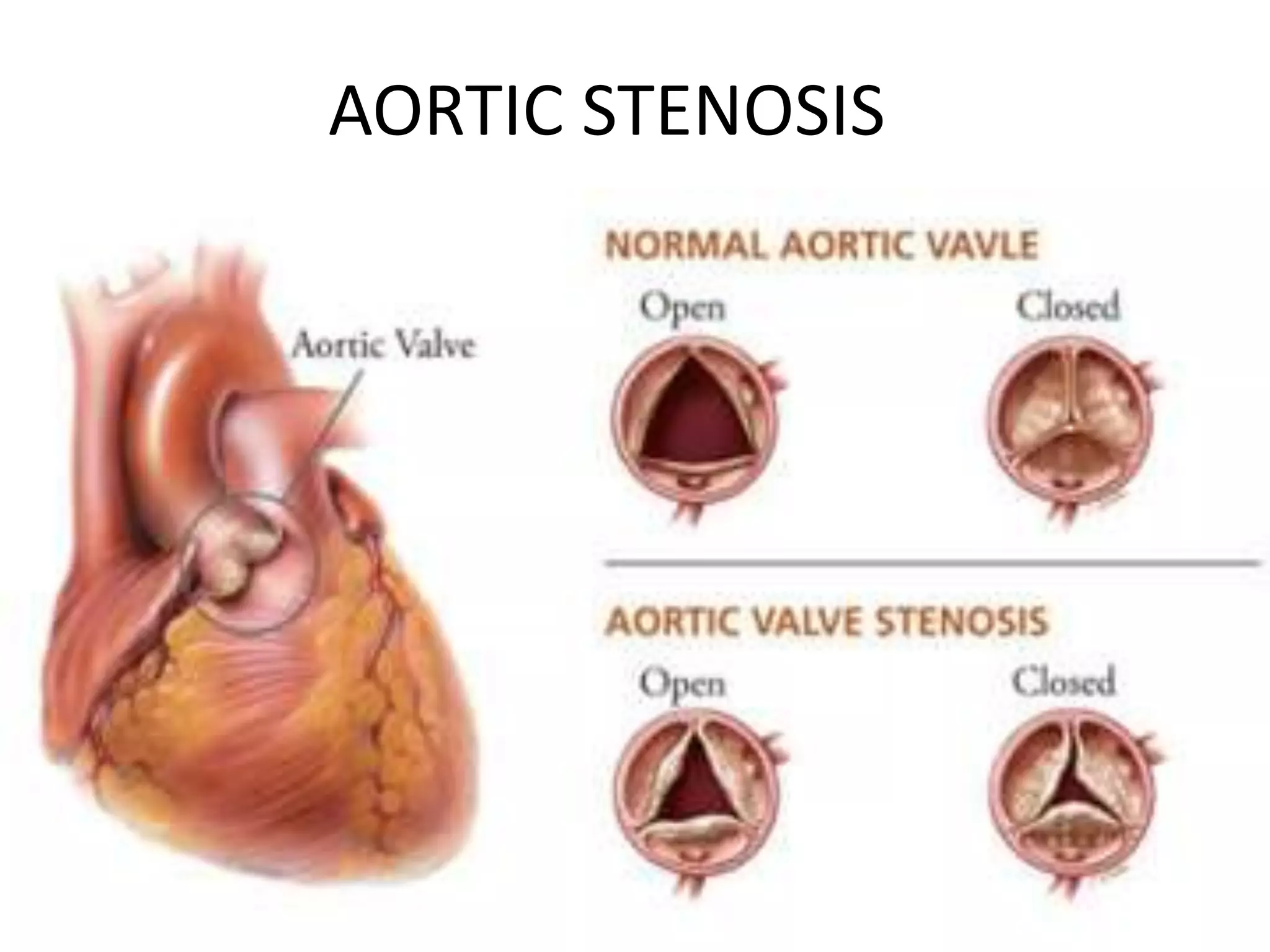

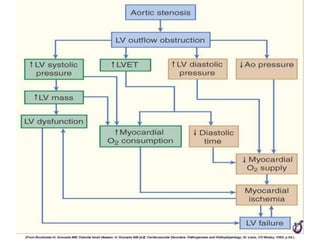

1) Aortic stenosis occurs when the aortic valve narrows, obstructing blood flow from the heart into the aorta. 2) It has several causes, including congenital bicuspid valve issues, calcification of normal or rheumatic valves, and rarely atherosclerosis. 3) Symptomatic patients have a poor survival without valve obstruction relief, with average survival of 1-3 years after symptom onset. Asymptomatic patients have an excellent long-term prognosis but severity increases gradually over 10-15 years.























































































