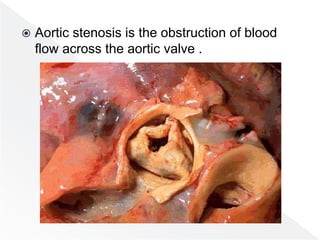
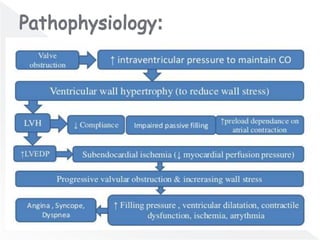
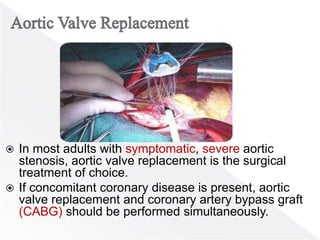
Aortic stenosis is characterized by obstruction of blood flow at the aortic valve, often resulting from either congenital or acquired conditions, with typical symptoms emerging gradually over years. Diagnosis primarily relies on two-dimensional and Doppler echocardiography, while the only definitive treatment is aortic valve replacement, either surgically or percutaneously. Asymptomatic patients generally have a good prognosis, but symptomatic individuals experience significantly higher mortality rates, and management strategies must consider individual patient risks and comorbidities.