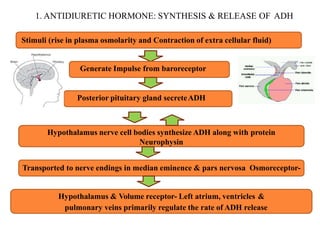
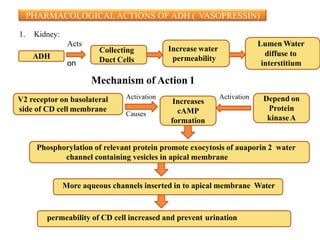
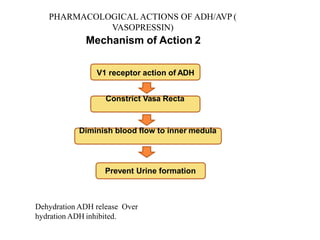
This document discusses antidiuretic drugs, which reduce urine volume. It describes various classes of antidiuretic agents including antidiuretic hormone (ADH/vasopressin), thiazide diuretics, and miscellaneous drugs. ADH is synthesized and released by the posterior pituitary gland and acts on V1 receptors in blood vessels and V2 receptors in kidney collecting ducts to increase water permeability and reduce urine volume. Desmopressin is a synthetic ADH analogue used to treat diabetes insipidus and bedwetting. Side effects of ADH include headache, flushing, and fluid retention. Thiazide diuretics and drugs like amiloride and indomethac