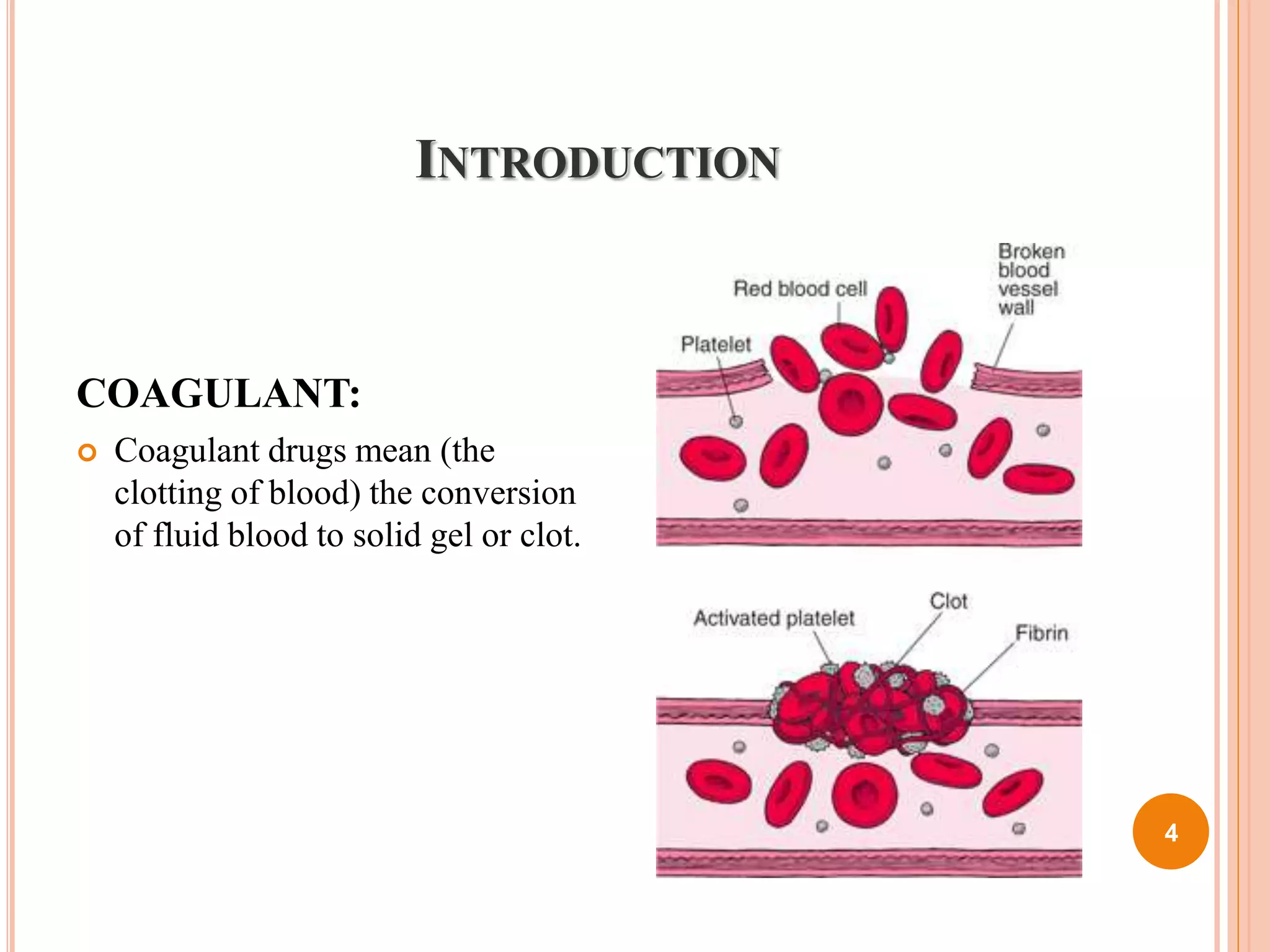
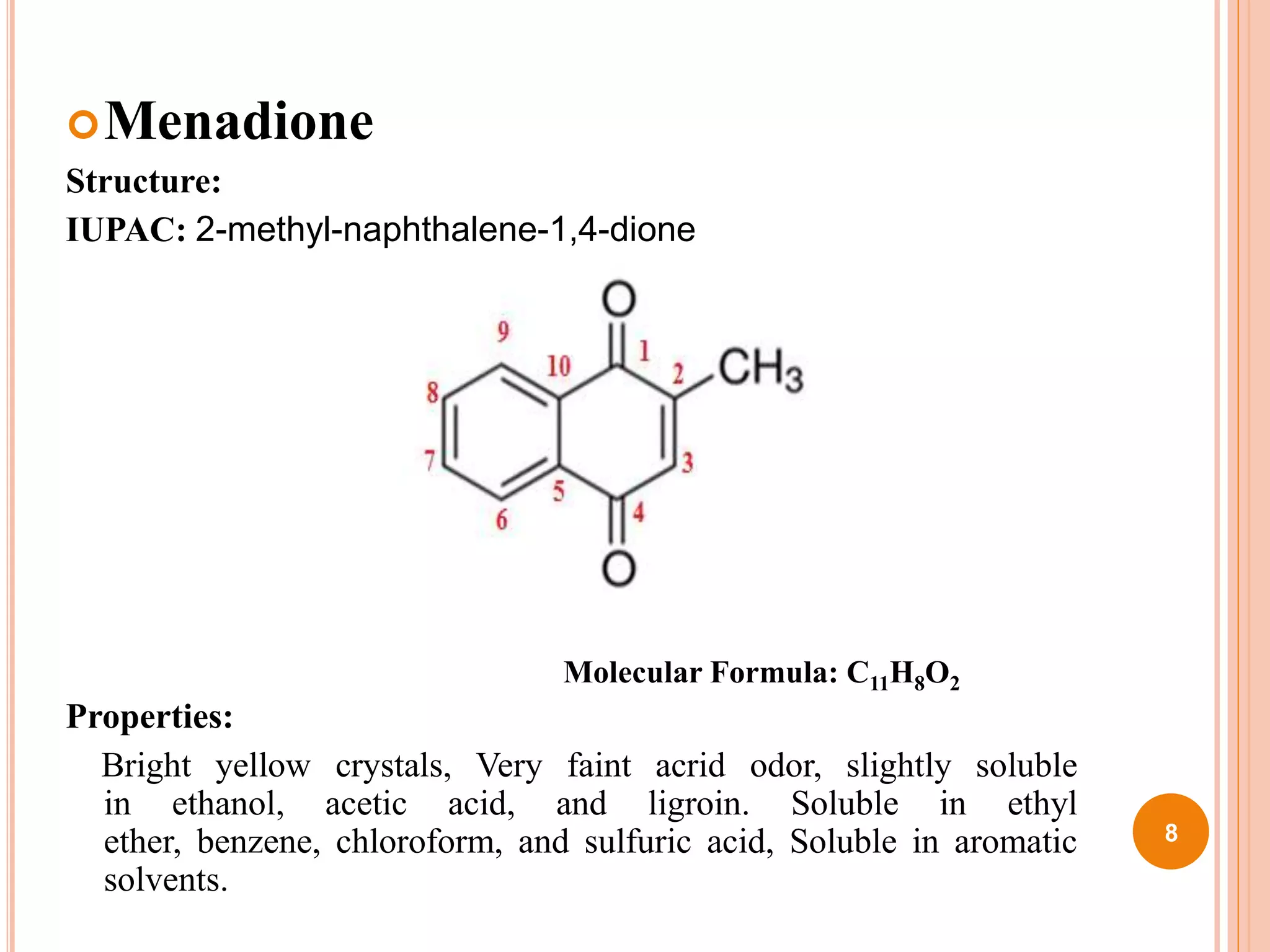
The document discusses coagulant and anticoagulant agents, including their classification, mechanisms of action, and therapeutic uses. It covers specific drugs like vitamin K and warfarin, detailing their structures, pharmacokinetics, adverse reactions, and dosages. Additionally, it provides references for further reading on medicinal chemistry.

















































![1.Hemodynamic and electrophysiology [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/1-240116072053-6f97ce28-thumbnail.jpg?width=640&height=640&fit=bounds)