Downloaded 83 times



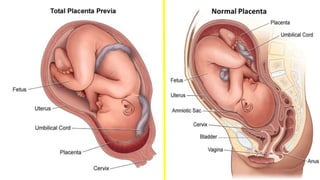
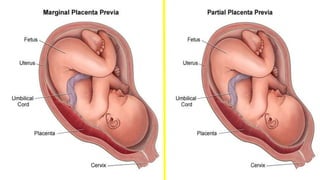

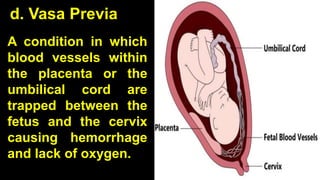


The document provides an overview of the placenta, its role in pregnancy, and details various placental abnormalities and associated hemorrhagic complications. It highlights conditions such as antepartum hemorrhage, placental previa, and placental abruption, including their causes, risk factors, symptoms, and management strategies. The information emphasizes the medical importance of monitoring and addressing these complications for maternal and fetal health.




































![obstetric 1 antinatal care for midwifery].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604190707-264c2efa-thumbnail.jpg?width=640&height=640&fit=bounds)
![obstetric 2 lecture note for health].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604192427-51f7250b-thumbnail.jpg?width=640&height=640&fit=bounds)

















































