
Recommended
More Related Content
Similar to AMYLOIDOSIS
Similar to AMYLOIDOSIS (20)
Recently uploaded
Recently uploaded (20)
AMYLOIDOSIS
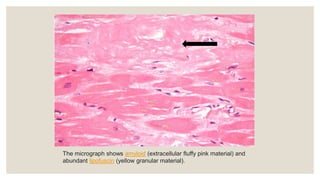
- 1. The micrograph shows amyloid (extracellular fluffy pink material) and abundant lipofuscin (yellow granular material).
- 2. Amyloid positivity with Congo red stain. Polarized microscopy reveals apple- green birefringence for amyloid
- 3. AMYLOIDOSIS PRESENTER- DR ZUBIY SUHA MODERATOR- DR PRINCY SOMAN
- 4. OBJECTIVES- ◦ Introduction ◦ Physical properties ◦ Chemical properties ◦ Pathogenesis ◦ Classification ◦ Morphology ◦ Diagnosis ◦ Stains ◦ Summary ◦ References
- 5. AMYLOID • Amyloid is the eosinophilic amorphous extracellular insoluble misfolded fibrillar protein. • Deposition of this extracellular amyloid protein in various organs and tissues is known as Amyloidosis. • Different diseases of various etiopathogenesis may show amyloidosis
- 6. PHYSICAL PROPERTIES ELECTRON MICROSCOPY ◦ The fibrils are arranged in random array and are nonbranching ◦ Insoluble ◦ Linear ◦ Rigid ◦ 7-10 nm diameter.
- 7. PHYSICAL PROPERTIES ON X-RAY CRSTALLOGRAPHY AND INFRA RED SPECTROSCOPY • Each fibril consists of β pleated sheet polypeptide chains • Congo red dye binds to these fibrils and produces classic apple green birefringences under polarized light
- 8. CHEMICAL PROPERTIES Amyloid composed of 2 main types of amyloid Fibril protein - 95% of amyloid material consists of fibril proteins. Non-fibrillar component- 5%- P component with other proteins like apolipoprotein, glycosaminoglycans Chemically, 2 major forms of amyloid fibrils-AL and AA
- 14. AMYLOIDOSIS MORPHOLOGY ◦ Amyloidosis of different organs show variation in morphologic pattern, general features are- ◦ GROSS-affected organ is large, grey, waxy, and rubbery (firm in consistency) ◦ MICROSCOPY- deposits are always extracellular, begins between cell close to the basement membrane and are amorphous, eosinophilic
- 15. AMYLOIDODIS OF KIDNEY ◦ Most common and serious form ◦ GROSS- kidneys maybe normal sized, enlarged or shrunken in advance cases because of ischemia ◦ C/S- pale, waxy, translucent ◦ MICROSCOPY- amyloid deposit primarily in glomeruli, but arteries, arterioles and peritubular tissue are also affected
- 16. AMYLOIDODIS OF SPLEEN ◦ 2 patterns of deposition ◦ SAGO SPLEEN- MC the amyloid deposition is limited to splenic follicles, resulting in gross appearance of moderately enlarged spleen dotted with gray nodules ◦ LARDACEOUS SPLLEN- Amyloid involves the walls of splenic sinuses and connetive tissue framework in the red pulp. Fusion of early deposits give rise to large, map like areas of amyloidosis
- 17. AMYLOIDODIS OF LIVER • It may cause enlargement, pale, waxy and firm. • Histologically, amyloid deposits first appear in the space of Disse.(space between hepatocytes and sinusoidal endothelial cells) • Normal liver function is usually preserved.
- 18. AMYLOIDODIS OF HEART • It may produce arrhythmias due to deposition in conduction system. • In localized form, deposits seen in left atrium • Amyloid first deposits in subendocardial areas of atrium. • Most common cause of death is cardiac failure. ◦ GROSS- heart is enlarged and firm ◦ Epi/endocardium and valves show tiny nodules ◦ MICROSCOPY- focal subendocardial accumulations, in primary form, deposits are seen around myocardial fibres in ring forms also known as ring fibres
- 19. AMYLOIDODIS OF BRAIN ◦ Diseases A/W senile cerebral amyloidosis are Alzheimers disease, Downs syndrome, Creutzfeldt Jakob disease, kuru, mad cow disease ◦ Alzheimer's disease and other neurodegenerative disorders belong to family of protein misfolding diseases, characterized by protein self-aggregation and deposition ◦ In vivo detection of amyloid plaques and neurofibrillary tangles in the brain enables early identification of AD
- 20. When to suspect amyloidosis…..? ◦ Nephrotic range proteinuria with or without renal insufficiency ◦ Unexplained kidney failure ◦ Non-dilated cardiomyopathy ◦ Peripheral or autonomic neuropathy ◦ Hepatomegaly or splenomegaly ◦ Malabsorption
- 21. Diagnosis ◦ Iodine staining of amyloid ◦ -means starch like - painting on C/s with iodine – yellow color, which is transformed to blue violet after application of sulfuric acid(acidifies iodine) – ◦ This method was used to demonstrate cellulose or starch
- 22. DIAGNOSIS ◦ Presence of amyloid- -Evaluation of organ involvement (in-vivo test and imaging) -Tissue biopsy and its histology -Congo red staining ◦ Type of amyloid- -Immunohistochemistry ◦ Mutation type - amino acid sequence analysis Amyloid AAntibody Immunohistochemistry on a FFPE Kidney Tissue
- 23. TISSUE BIOPSY ◦ Subcutaneous fat aspiration(provides enough material from aspiration)rectal biopsy ◦ Gums ◦ Bone marrow ◦ Others- kidneys, nerves, heart, liver ◦ Organ biopsy- if subcutaneous fat investigation did not provide diagnosis ◦ Kidney biopsy to determine the cause of nephrotic syndrome
- 25. CONGO RED STAIN Steps of staining • Deparaffinize. • Pass through graded alcohol to bring in water • Rinse in distilled water: 10–15 dip • Stain by Mayer’s haematoxylin • Blueing by running tap water • Wash in distilled water • Alkaline alcohol sodium chloride solution: 20 min • Alkaline Congo red: 20 min • Rapid dehydration • Clear in xylene • Mount. Principle- Congo red intercalates between the parallel fibrils of the amyloid protein and forms a non-polar hydrogen bond
- 26. CONGO RED- Results: ◦ With the light microscope, amyloid deposits are red to pink-red, nuclei are blue ◦ Amyloid deposits show an “apple- green” birefringence with the polarizing microscope. ◦ Nuclei of inflammatory cells, and granular basophilic debris associated with vacuoles, stain dark blue/black Renal AA amyloidosis
- 27. THIOFLAVINE T STAIN • Thioflavine T is a very sensitive technique. Principle- This cationic benzothiazole dye increases in fluorescence upon binding to the stacked β sheets of amyloid fibrils • Not a specific stain for amyloid. Result- • Fluorescence microscope : Bright yellow fluorescence
- 28. OTHER STAINS •Metachromatic techniques methyl crystal violet crystal violet methyl green -imparts rose pink color. • Low sensitivity • Lack specificity ◦ • Van gieson- khakhi color ◦ • PAS- pink
- 29. OF VARIOUS AMYLOID STAININGSUMMARY METHODS
- 30. Identify ? Seen in ? Type of amyloid ? Neurofibrillary tangles Alzheimers disease A beta amyloid
- 31. First described by- Term first used by-based on color after staining with iodine Later recognized as protein by- Rudolf Virchow Karl von Rokitansky Friedrich August Kekule
- 32. REFERENCES Kumar V, Abbas A, Aster JC, Deyrup AT, editors. Robbins & Kumar Basic Pathology. 11th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2022. Suvarna KS, Layton C, Bancroft JD. Bancroft’s theory and practice of histological techniques. 8th ed. London, England: Elsevier Health Sciences; 2018. Muchtar E, Dispenzieri A, Magen H, Grogan M, Mauermann M, McPhail ED, et al. Systemic amyloidosis from A (AA) to T (ATTR): a review. J Intern Med. 2021;289(3):268–92. Picken MM. The pathology of amyloidosis in classification: A review. Acta Haematol. 2020;143(4):322–34
Editor's Notes
- Peripheral_variant_of_calcifying_epithelial_odontogenic_tumor_with_clear_cell_changes_An_enigma
- • Different diseases of variable etiopathogenesis may show amyloidosis
- An electron micrograph of amyloid fibrils in section of human amyloidotic spleen
- Apple-green birefringence under polarized light. Positive lambda light chain stain in a glomerulus.
- Non-fibrillar componenet
- Idiopathic MM, B cell lymphoma, Monoclonal gammopathies Mutant forms- ATTR, AB2M from B2 microglobuln, AB in Alzheimers APrP in senile cerebral amyloidosis Acal in procalcitonin
- AIAPP- islet amyloid polypeptide APP-amyloid precursor protein SAA- serum amyloid associated
- breast
- It is the most common & most serious feature of renal disease. Deposits in the kidney mostly in secondary amyloidosis. Amyloidosis deposition occurs primarily in glomeruli. Glomerulus develops focal deposits within mesengial matrix & diffuses the basement membranes of capillary loops. It results in proteinuria & nephrotic syndrome
- Lard-fat of pig
- Later as deposits increase they compress the hepatocytes and eventually liver cells shrunk and atrophied Later, disappearance of hepatocytes occur due to pressure atrophy
- AL amyloid binds & inactivates factor X causes bleeding disorder.
- Neurofib tangles are abnormal accumulations of a protein called tau
- Protein >3g in 24 hours
- Lugols iodine- iodine-5%, potassium iodide-10%
- formalin fized paraffin embedded Antibodies can identify special epitopes on amyloid fibrils and p component Extracellular, Cytoplasmic Serum amyloid A (SAA) proteins are a family of apolipoproteins associated with high-density lipoprotein (HDL) in plasma. Different isoforms of SAA are expressed constitutively (constitutive SAAs) at different levels or in response to inflammatory stimuli (acute phase SAAs). These proteins are produced predominantly by the liver. The conservation of these proteins throughout invertebrates and vertebrates suggests that SAAs play a highly essential role in all animals. Acute-phase serum amyloid A proteins (A-SAAs) are secreted during the acute phase of inflammation
- Each fibril consists of β pleated sheet polypeptide chains • Congo red dye binds to these fibrils and produces classic apple green birefringences under polarized light The method obviates the need for a differentiation step by the inclusion of a high concentration of sodium chloride. This reduces background electrochemical staining whilst enhancing hydrogen bonding of Congo red to amyloid, resulting in a progressive and highly selective technique Bleuing- convert the soluble red component of H into insoluble blue
- , other tissue elements are unstained.
- using BG12 exciter filter and K 530 barrier filterGlomerulus with extensive amyloid deposition detected by strong fluorescence with thioflavin T stain. Note, also, staining of adjacent arteriolar wall. Thioflavin T stain viewed under fluorescent light. Magnification ×750 (a) Eosinophilic, amorphous (hyaline) material corresponding to areas with amyloid deposition noted in the three renal compartments: glomerulus, interstitium, and extraglomerular vessels. Hematoxylin and eosin stain, original magnification ×350. (b) Distinct fluorescence highlighting amyloid deposits in the three renal compartments: glomerulus, interstitium, and extraglomerular vessels. Thioflavin T stain, original magnification ×350
- SIRIUS RED Similar to congo red • Gives more intense staining reaction-photographic purpose • Gives green birefringence with polarized light without any fluorescence Collagen-red, nuclei-blue, rbc- yellow. Elastin-blue/black