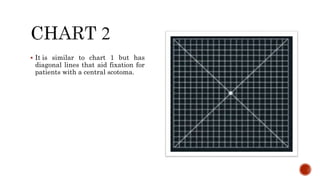
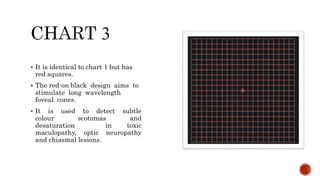
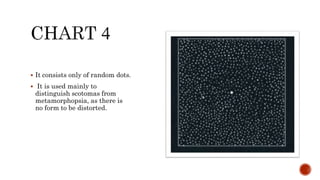
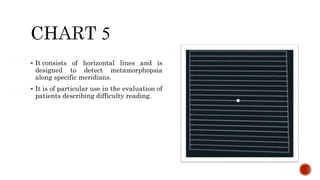
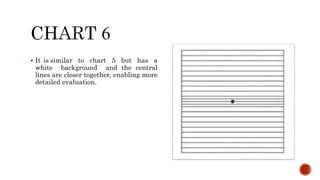
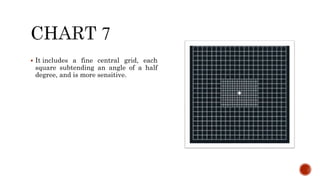
The document discusses the Amsler grid, which is used to monitor central visual field and detect macular disease. It consists of a grid with a central fixation dot that is viewed to check for distortions, blurred spots, or missing areas that may indicate problems in the macula. The document describes the different types of Amsler grids and how to properly administer the test, noting things like maintaining fixation, checking all corners and sides of the grid, and having the patient draw any anomalies observed. Abnormal results on an Amsler grid can provide clues to macular diseases, optic neuropathies, or other central visual field defects.