Downloaded 583 times










![14
CHART NO 4:
• This chart has no lines to distort; instead it
consists of small white dots randomly
distributed over a black background like stars in
the sky.
• Amsler hoped that the patient with one or more
paracentral scotomas may be able to delineate
the area[s] of involvement more easily with this
chart.
• But its credibility is doubtful since the
background and scotoma use to appear same in
color for the observer may result in false results](https://image.slidesharecdn.com/amslergridchart-140509023115-phpapp02/75/Amsler-grid-chart-14-2048.jpg)






![22
CLINICAL IMPLICATIONS
• Disturbances that appear on the Amsler grid should
alert the clinician to the possibility of either acute
or longstanding disease of the retina, choroid, optic
nerve, anterior visual system, visual pathways and
cortex.
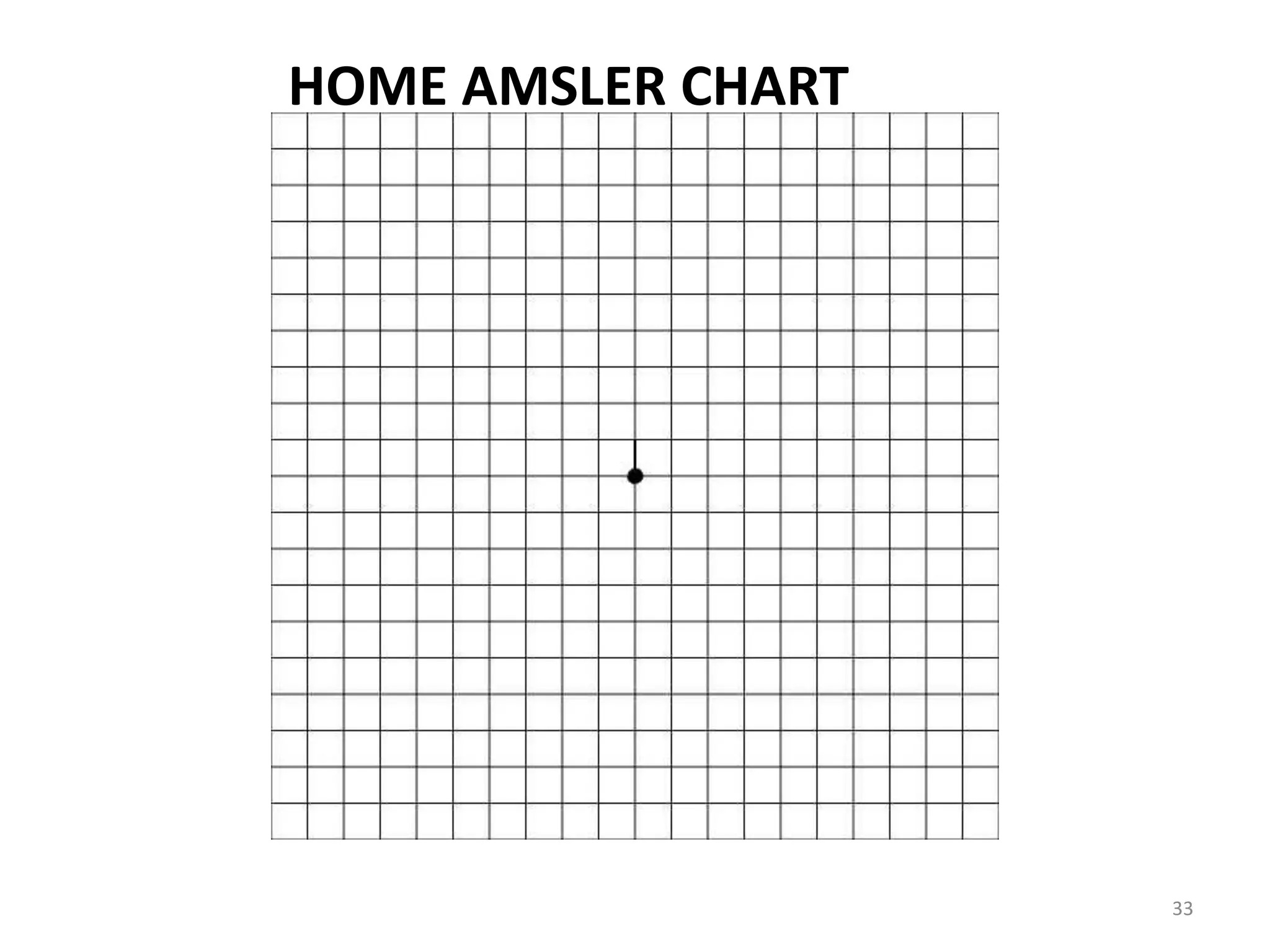
• The clinician should consider dispensing an Home
Amsler grid chart [Black lines in white background]
with complete instructions for self-assessment to
three categories of patients.](https://image.slidesharecdn.com/amslergridchart-140509023115-phpapp02/75/Amsler-grid-chart-22-2048.jpg)








![34
• The first category is the patient with progressive
disease, such as toxic maculopathy or atypical
retinitis pigmentosa [field defect starts from center
to periphery] , who is predisposed to developing
significant alterations in the functional vision over
time.
• The second category is the patient with active
disease, such as optic neuritis or macular
neuroretinopathy, whose visual acuity may improve
or worsen within a relatively short time span.](https://image.slidesharecdn.com/amslergridchart-140509023115-phpapp02/75/Amsler-grid-chart-34-2048.jpg)


![(4) Patient should be always looking directly at
the central white dot at all times.
(5)If patient notice any [new] missing or
distorted areas, he/she should mark them
with a pencil.
(6) Patient should report the clinician along with
Home Amsler chart used as soon as possible
for any new symptoms found with the chart.](https://image.slidesharecdn.com/amslergridchart-140509023115-phpapp02/75/Amsler-grid-chart-37-2048.jpg)

The document describes the Amsler grid chart, which was developed in 1920 by Dr. Marc Amsler to test for central vision disorders. It consists of a grid pattern with white lines on a black background that is used to evaluate the macula. Patients are asked a series of questions while viewing the chart to check for blurriness, distortions, or missing areas that could indicate conditions like macular degeneration or retinal detachment. The document outlines the purposes and procedures for several variations of the Amsler grid and provides instructions for patients to perform self-examinations at home in order to monitor eye conditions.














































































