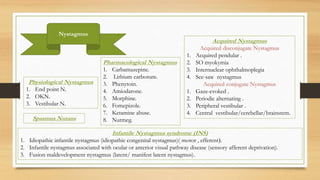
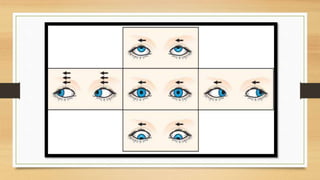
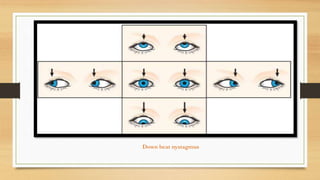
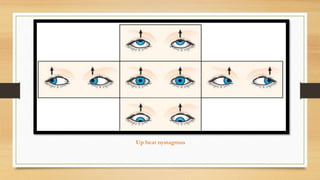
Nystagmus refers to involuntary eye oscillations. There are several types of nystagmus including physiological nystagmus seen with extreme gaze, optokinetic nystagmus induced by moving targets, and vestibular nystagmus caused by altered vestibular input. Infantile nystagmus syndrome includes idiopathic congenital nystagmus and nystagmus associated with visual pathway diseases. Acquired nystagmus can be conjugate seen with brainstem and cerebellar diseases, or disconjugate like acquired pendular nystagmus. Treatment is difficult but may include drugs, optical devices, or surgery to stabilize or move the null position.