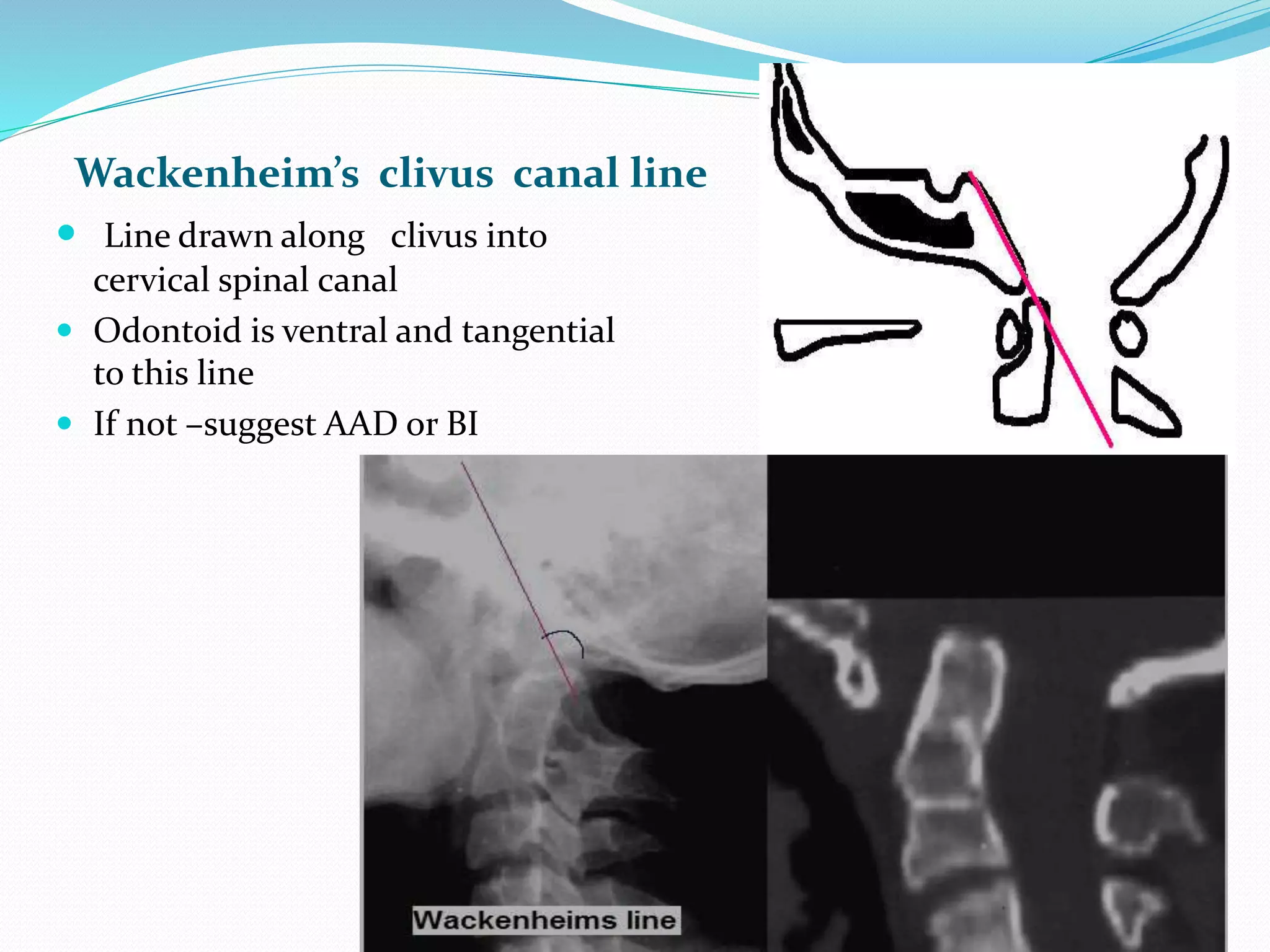
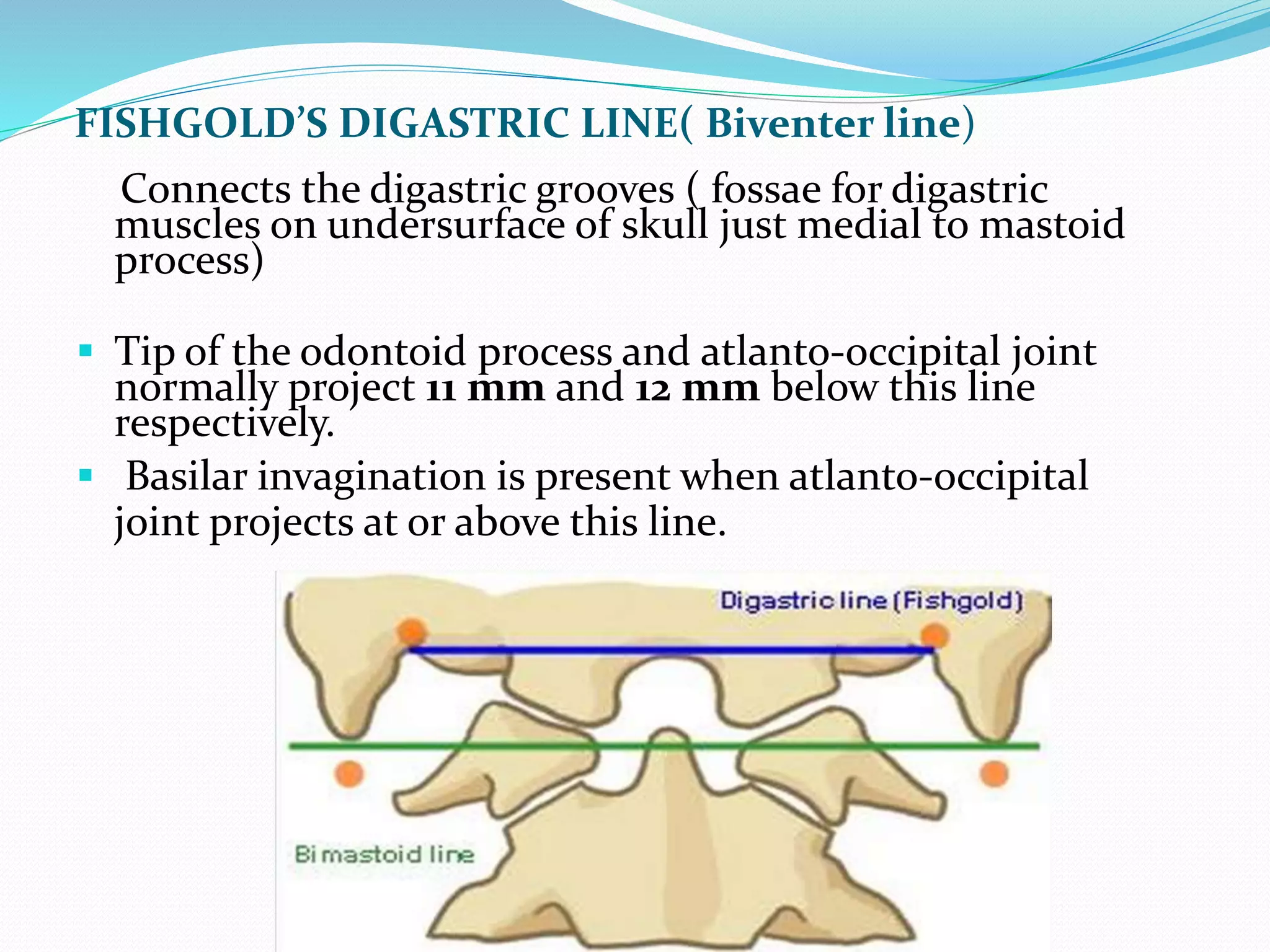
This document provides an overview of the anatomy, classification, and clinical features of craniovertebral junction anomalies. It begins by describing the normal anatomy of the occiput-C1-C2 articulations and ligaments. It then discusses various congenital and acquired bony and soft tissue anomalies that can affect the craniovertebral junction, including occipitalization, basilar invagination, atlantoaxial instability, and dens dysplasia. The document also outlines methods for evaluating craniovertebral junction anomalies using radiography, CT, MRI, and craniometric measurements. It concludes by describing clinical signs and symptoms as well as treatments for different types of craniovertebral junction abnormalities.



















































































































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)
































