Downloaded 25 times
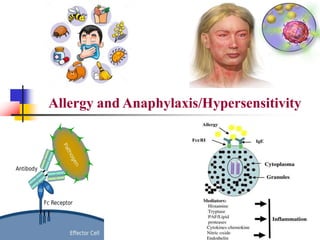
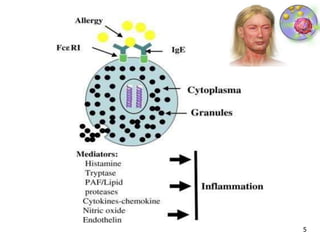
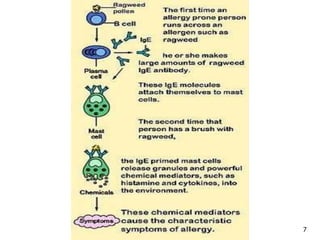
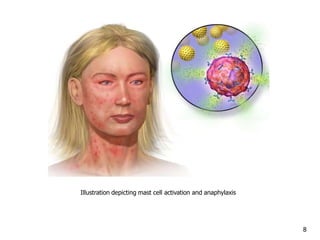
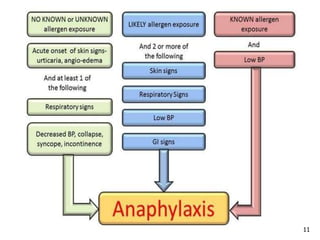
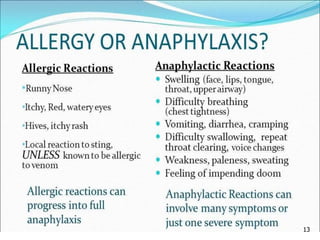
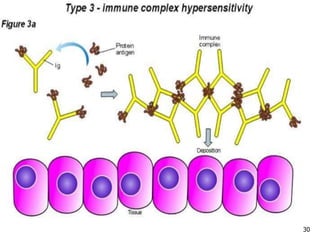
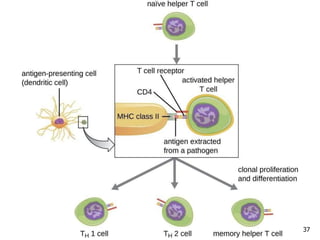
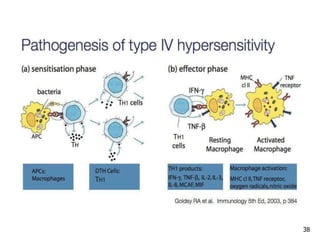
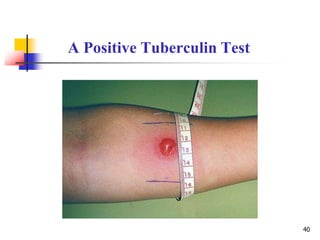
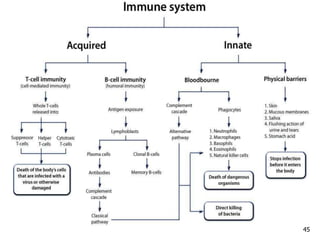
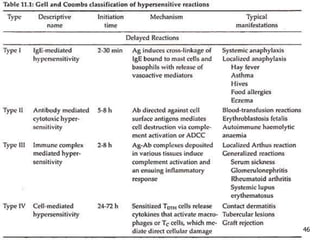
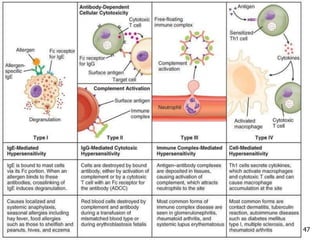

Allergy and Anaphylaxis/Hypersensitivity document discusses: 1. Allergies are immune system disorders caused by hypersensitivity to allergens like foods, pollens, or dusts. Anaphylaxis is a severe, potentially life-threatening allergic reaction affecting multiple body systems. 2. The four types of hypersensitivity reactions are: Type I involves IgE antibodies and causes immediate allergic reactions. Type II involves IgG/IgM antibodies attacking cell surfaces. Type III involves immune complex formation and complement activation causing tissue damage. Type IV is cell-mediated and involves T lymphocytes responding to antigens days later. 3. Anaphylaxis differs from other allergic reactions in affecting multiple























































































