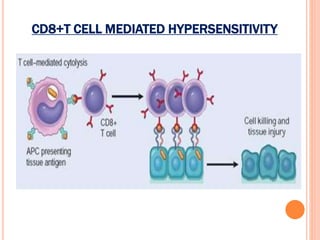
This document discusses Type IV hypersensitivity reactions, which are mediated by T cells. It describes how CD4+ T cells can differentiate into Th1 and Th17 effector cells that promote inflammation through cytokine production. It also explains the three pathways through which CD8+ T cells exert their cytotoxic effects: cytotoxin mediated killing, Fas-mediated apoptosis, and cytokine production. Finally, it provides several clinical examples of conditions involving CD4+ and CD8+ T cell-mediated hypersensitivity, such as tuberculosis and autoimmune diseases.