Download as PDF, PPTX
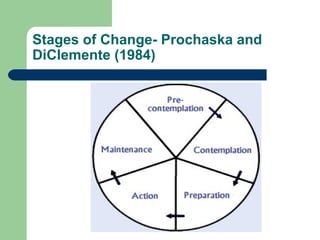
![Stages of Change- Prochaska and
DiClemente (1984)
Contemplation
Ambivalent about change:" Sitting on the fence"
Not considering change within the next month
[Miller and Rollnick (1991)]
Techniques
Validate lack of readiness
Clarify: decision is theirs
Encourage evaluation of pros and cons of
behavior change
Identify and promote new, positive outcome
expectations](https://image.slidesharecdn.com/alcoholdependencesyndromepdf-120426022731-phpapp01/85/Alcohol-dependence-syndrome-pdf-6-320.jpg)





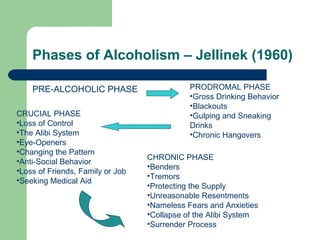
The document summarizes Jellinek's phases of alcoholism which include a pre-alcoholic phase, prodromal phase, crucial phase, chronic phase. It also discusses Prochaska and DiClemente's stages of change model for addiction which includes precontemplation, contemplation, preparation, action, maintenance, and relapse stages. Finally, it outlines different treatment approaches for alcohol dependence like motivational interviewing, behavioral interventions, relapse prevention, psychosocial treatments, and functional analysis.






































































































