Downloaded 1,458 times
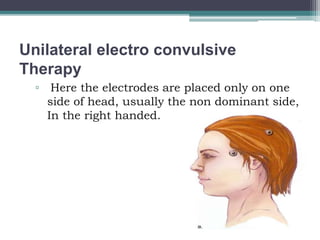
This document discusses electroconvulsive therapy (ECT), including its definition, types, indications, contraindications, side effects, and procedures. ECT involves inducing a seizure through electrical stimulation of the brain under anesthesia to treat various mental health conditions such as severe depression, bipolar disorder, and schizophrenia. It can cause short-term memory loss and other potential side effects but is considered an effective treatment when other options have failed. The document provides detailed information on administering and monitoring ECT according to established guidelines.