Downloaded 38 times

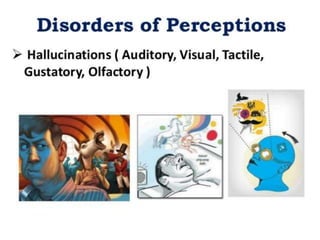
![ETIOLOGY
1) BIOLOGICAL THEORIES
Biochemical theories
Dopamine Hypotheses An excess of
Dopamine – Dependent neuronal activity in the
brain may cause schizophrenia
Other Biochemical Hypotheses Abnormalities
in the Neuro - transmitters ( Nor epinephrine,
Serotonin, Acetylcholine & Gamma – amino
butyric acid [GABA] ).](https://image.slidesharecdn.com/schizophrenia-200405130143/85/Schizophrenia-11-320.jpg)
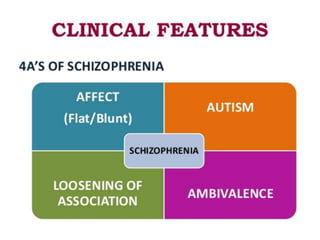
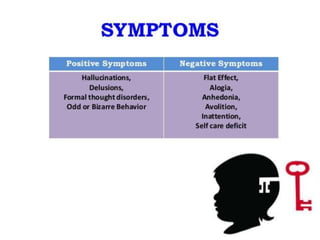
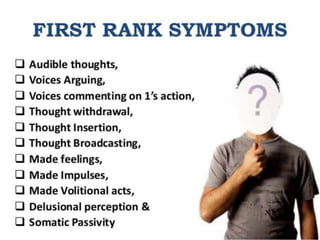
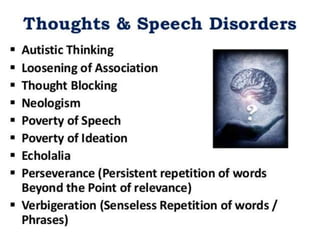



1) Schizophrenia is a psychotic disorder characterized by distortions in thinking, perception, and affect. It was first described in 1896 and the term was coined in 1911. 2) Schizophrenia is classified by symptoms in the DSM-IV and ICD-10 and includes delusions, hallucinations, disorganized speech/behavior, and negative symptoms. 3) Etiology may include biological, genetic, developmental, and environmental factors. Treatment involves antipsychotic medication which can cause side effects.