Downloaded 158 times
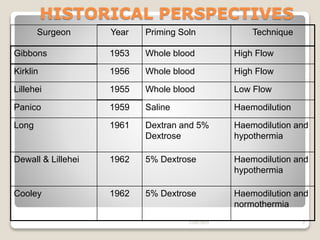
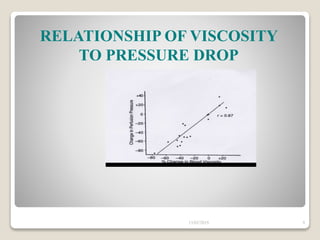
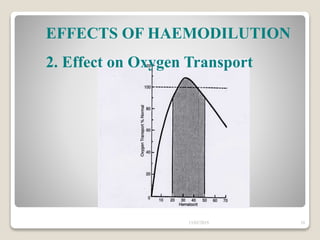
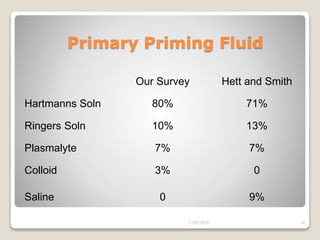
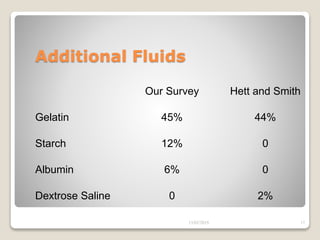
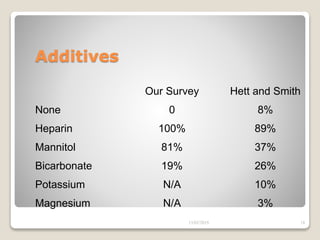
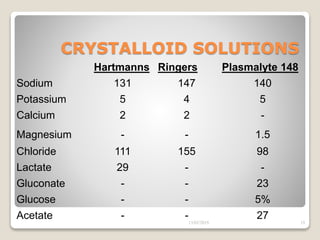

This document discusses the history and techniques of priming fluids and hemodilution in cardiopulmonary bypass. It notes that early surgeons used whole blood for priming, while later techniques incorporated saline and dextrose solutions to enable hemodilution. Hemodilution provides benefits like reduced blood viscosity and improved oxygen delivery, but can cause issues like decreased oxygen carrying capacity if taken to an extreme. The document examines various priming fluid options and how hemodilution affects viscosity, oxygen transport, and hematocrit. Overall, priming fluids and controlled hemodilution have advanced CPB by enabling adequate organ perfusion in difficult circumstances and reducing complications while conserving blood.
































![Fluid manage 최종[1]](https://cdn.slidesharecdn.com/ss_thumbnails/fluidmanage1-141006002453-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)






















































