Downloaded 20 times







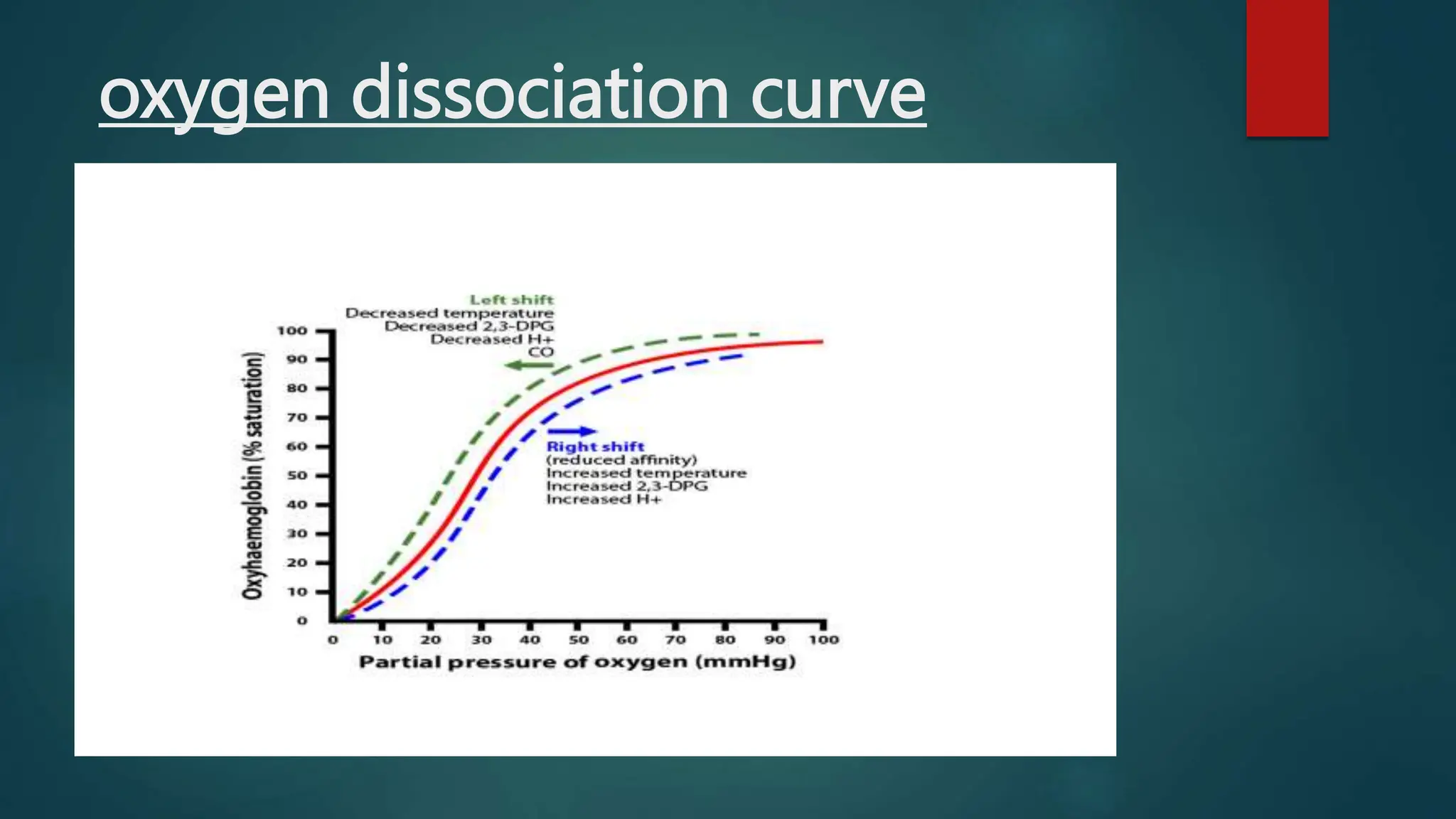
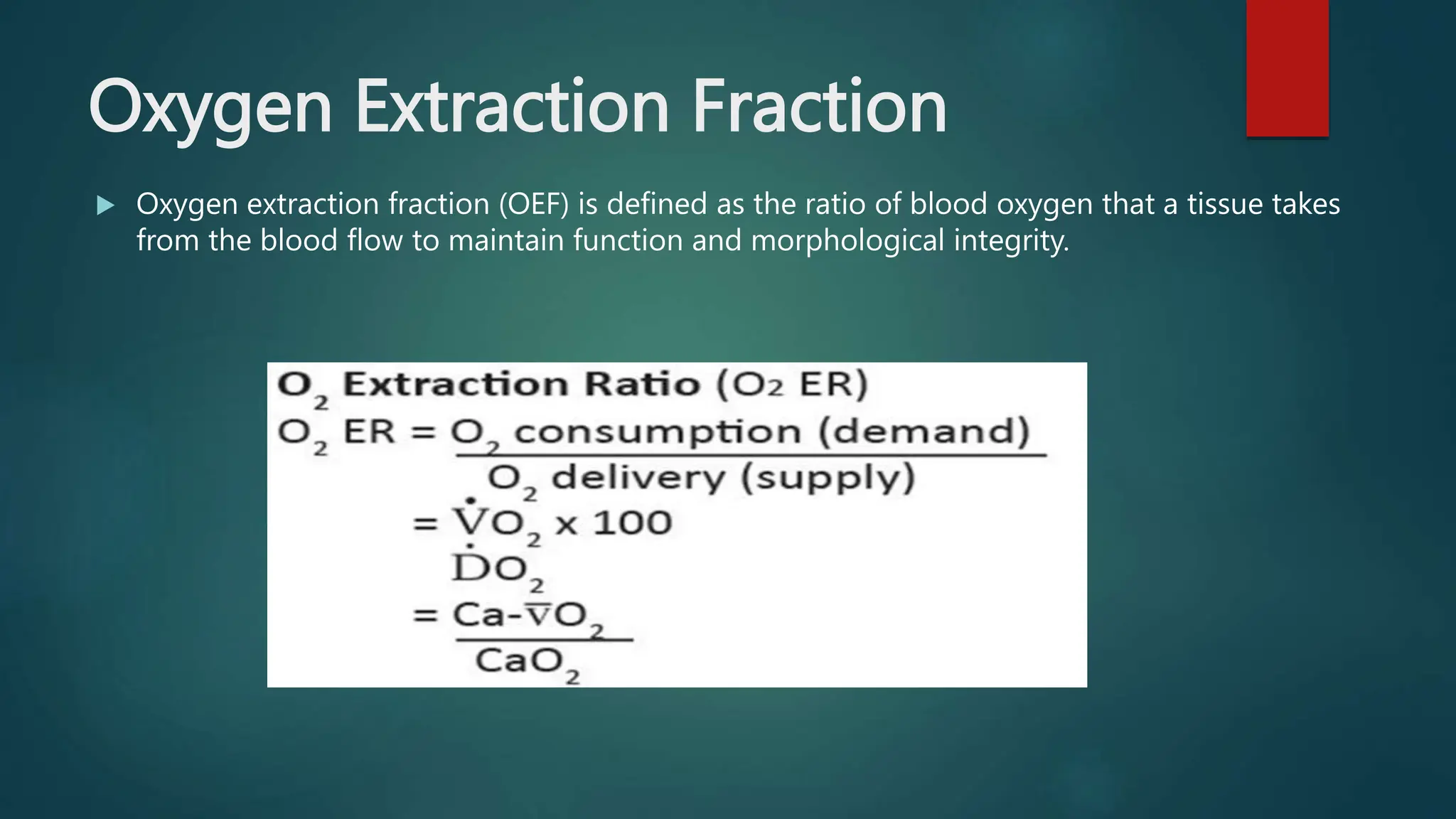





Goal directed perfusion (GDP) aims to optimize hemodynamics during cardiopulmonary bypass based on goal directed therapy principles. Adequate perfusion depends on factors like blood flow, fluid balance, and temperature that influence oxygen delivery and uptake in tissues. The critical oxygen delivery threshold is 270 ml/min/m2. Key parameters in GDP include cardiac output, hemoglobin, arterial oxygen saturation, and partial pressure of oxygen. While oxygen uptake is initially independent of oxygen delivery, it becomes dependent when delivery falls below the critical threshold, leading to anaerobic metabolism and lactate production. The maximum oxygen extraction ratio is 60-70%. A competent perfusionist integrates multiple parameters to ensure adequate perfusion tailored to























































































