Downloaded 837 times
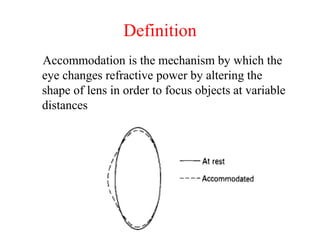




























































(1) Accommodation is the mechanism by which the eye changes refractive power by altering the shape of the lens to focus on objects at different distances. (2) Theories of accommodation include the relaxation theory of Helmholtz which proposes that contraction of the ciliary muscle relaxes the suspensory ligaments of the lens allowing it to take on a more spherical shape. (3) Accommodative anomalies include decreased accommodation seen in presbyopia and other conditions, as well as increased accommodation seen in conditions like accommodative excess or spasm.























































































