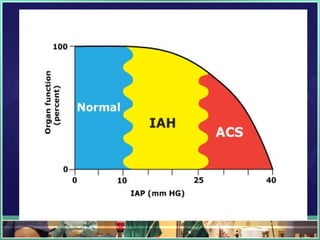
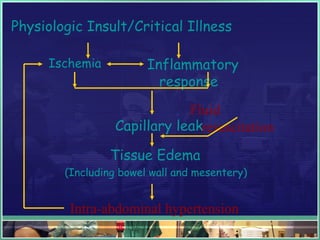
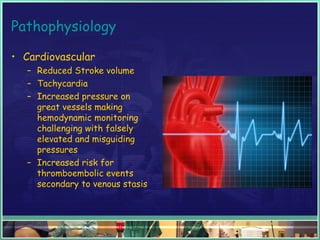
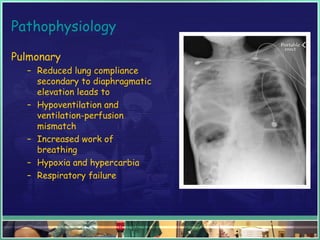
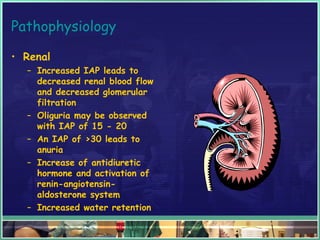
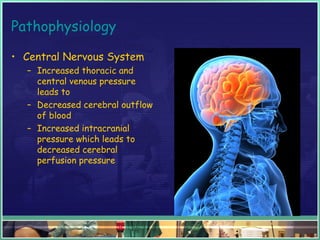
This document discusses abdominal compartment syndrome (ACS). It defines ACS as a sustained intra-abdominal pressure (IAP) above 20 mmHg associated with new organ dysfunction. Normal IAP is 5-7 mmHg. Intra-abdominal hypertension is defined as IAP above 12 mmHg and is graded. ACS can result from primary abdominal causes or secondary extra-abdominal causes and leads to organ dysfunction through reduced blood flow. Accurate IAP monitoring via bladder pressure is important for early detection and treatment to prevent organ failure.











![Abdominal compartment syndrome[1]](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalcompartmentsyndrome1-121012075429-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












