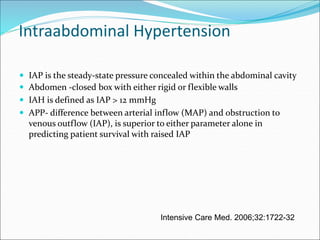
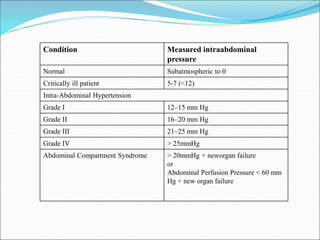
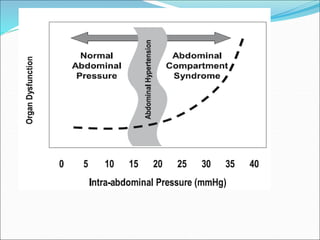
A 54-year old female underwent a major surgery for carcinoma ovary with significant blood loss requiring multiple transfusions. Post-operatively she developed signs of intra-abdominal hypertension including decreased urine output, elevated CVP and hypotension. Her intra-abdominal pressure was measured to be over 20 mmHg consistent with abdominal compartment syndrome, a condition where elevated intra-abdominal pressure compromises organ function. She required surgical decompression to relieve the pressure and allow organ recovery.























![Abdominal compartment syndrome[1]](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalcompartmentsyndrome1-121012075429-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































