
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Abdominal compartment syndrome
Similar to Abdominal compartment syndrome (20)
Recently uploaded
Recently uploaded (20)
Abdominal compartment syndrome
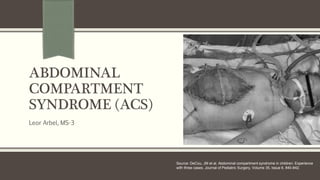
- 1. ABDOMINAL COMPARTMENT SYNDROME (ACS) Leor Arbel, MS-3 Source: DeCou, JM et al. Abdominal compartment syndrome in children: Experience with three cases. Journal of Pediatric Surgery, Volume 35, Issue 6, 840-842.
- 2. What is Abdominal Compartment Syndrome (ACS)? Refers to organ dysfunction caused by intraabdominal hypertension Tx can improve organ dysfunction, so it’s important to consider this diagnosis Primarily affects pts who are already very ill – thus, S/Sx of ACS can be mistakenly attributed to progression of the primary illness → heightened awareness of ACS is needed! Intra-Abdominal Hypertension (IAH) is not the same thing as ACS; IAH = sustained Intra-abdominal Pressure (IAP) ≥ 12 mmHg Note: IAP in critically ill pts between 5 – 7 mmHg is considered normal For research purposes, ACS = sustained IAP > 20 mmHg Clinically, however, there is no IAP value that reliably diagnoses ACS in all pts. Therefore, it is more helpful to think of ACS as IAH-induced new organ dysfunction That said, pts w/IAP < 10 mmHg generally do not have ACS and pts w/IAP > 25 mmHg usu do have ACS
- 3. Primary vs Secondary ACS Primary ACS Secondary ACS ▪ Due to abdominopelvic injury or disease ▪ Examples: Trauma, Hemoperitoneum, Pancreatitis ▪ Due to conditions that do NOT originate in abdominopelvic region but which require extensive fluid resuscitation (→ splanchnic reperfusion) ▪ Examples: Fluid resuscitation, Burns, Sepsis
- 4. Who gets ACS? ACS is MC seen in pts who are critically ill, but there is a wide variety in their underlying medical/surgical conditions. Examples include: TRAUMA – Injured pts in shock who need aggressive fluid resuscitation BURNS – Pts with burns involving >30% of body surface area ACS vs NEC vs Ischemic bowel SEPSIS – Along with other medical conditions that require extensive fluid resuscitation and are a/w 3rd spacing of fluids & tissue edema LIVER TRANSPLANTATION RETROPERITONEAL PATHOLOGIES – Eg ruptured AAA (8% of these pts develop ACS), pelvic fractures, pancreatitis POST-SURGICAL – Pts undergoing operations in which they are given large volume resuscitation, esp with crystalloid in the face of hemorrhagic or septic shock
- 5. Physiologic Manifestations of ACS Intra-abdominal Hypertension (IAH) can cause dysfunction in nearly every organ system, thereby causing ACS Table shows a summary of the key physiologic effects a/w elevated intra-abdominal pressure Physiologic deterioration frequently manifests as end-organ sequelae eg: ↓ urine output ↑ pulmonary inspiratory pressure ↓ cardiac preload ↑ cardiac afterload Source: UpToDate
- 6. Physiologic Manifestations of ACS (cont’d) This is a better visual representation of the effects discussed on the previous slide Source: Brunicardi FC, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. Trauma. Schwartz's Principles of Surgery, 10e (2014)
- 7. Signs & Symptoms Pt is usually critically ill, unable to communicate. Rarely, the pt is verbal & conveys symptoms of malaise, weakness, abdominal pain and bloating. Tensely distended abdomen Progressive oliguria Increased ventilatory requirements, acute pulmonary decompensation Hypotension Tachycardia Elevated JVP, JVD Hypoperfusion → cool skin, obtundation, lactic acidosis
- 8. Diagnosis Dx requires that IAP be measured. IAP cannot be reliably determined via physical exam, and S/Sx and imaging findings are also insufficient for Dx. IAP can be approximated by measuring the patient’s bladder pressure 50 mL saline instilled into bladder via aspiration port of Foley catheter with the drainage tube clamped 3-way stopcock and water manometer are placed at level of pubic symphysis Bladder pressure can then be viewed (in cm of water) on the manometer
- 9. Management No specific bladder pressure prompts therapeutic intervention (unless the pressure is > 35 mmHg) Emergent decompression is warranted when IAH reaches a level at which end-organ dysfunction is observed Decompression is usu performed operatively (decompressive laparotomy) In operative decompression with egress of the abdominal contents → temporary coverage using a subfascial sterile drape and Ioban application is placed over the abdominal viscera If significant intra-abdominal fluid is a primary component of the pt’s ACS (as opposed to bowel or retroperitoneal edema), decompression can be achieved non-operatively via Percutaneous Drain Most applicable to pts with major liver injuries Mortality is directly affected by the timing of decompression: 60% mortality if presumptive decompression 70% mortality if delayed decompression Nearly 100% mortality if no decompression
- 10. Operative Decompression Images from: Smith WR, Stahel P. Management of Musculoskeletal Injuries in the Trauma Patient.
- 11. Complications & Other Surgical Considerations Recognition of ACS and performance of damage control surgery have ↑ pt survival, but at the cost of an open abdomen Pts with an open abdomen lose btwn 500-2500 mL per day of abdominal effluent (albumin rich fluid). Appropriate volume compensation for this loss remains controversial, both wrt amount and type of replacement (crystalloid vs colloid). Interestingly, despite having a widely open abdomen, pts can develop recurrent ACS (this ↑ morbidity & mortality) Therefore, recommended to monitor bladder pressure q4hr. Significant increases in pressure may warrant repeat operative decompression Following resuscitation & management of specific injuries where applicable, goal of operative team is to close the abdomen as quickly as possible! Doing so promotes fascial closure and minimizes morbidity as well as cost of care. Delayed abdominal wall reconstruction = greater pt morbidity & resource invasive Advent of wound VAC technology has revolutionized fascial closure Authors used a sequential closure technique with the wound VAC device on constant fascial tension with return to the OR every 48 hrs until closure is complete with a success rate of 95% Mgmt requires frequent operative/percutaneous drainage of abscesses, fistula control and prolonged TPN
- 12. Sequential Closure Technique for Open Abdomen with Wound VAC Source: Brunicardi FC, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. Trauma. Schwartz's Principles of Surgery, 10e (2014) Authors’ sequential closure technique for the open abdomen
- 13. References DeCou, JM et al. Abdominal compartment syndrome in children: Experience with three cases. Journal of Pediatric Surgery, Volume 35, Issue 6, 840-842. Burlew Cn, Moore EE. Trauma. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. eds. Schwartz's Principles of Surgery, 10e New York, NY: McGraw-Hill; 2015. http://accessmedicine.mhmedical.com/content.aspx?bookid=980§ionid=59610848. Accesse d March 04, 2017. Gestring, M. Abdominal Compartment Syndrome in Adults. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on March 4, 2017).
Editor's Notes
- Image from: DeCou, JM et al. Abdominal compartment syndrome in children: Experience with three cases. Journal of Pediatric Surgery, Volume 35, Issue 6, 840-842.
- Note: For pts with severe burns, ACS must be distinguished from other abdominal pathologies seen commonly in this population such as Necrotizing Enterocolitis and ischemic bowel. As you can see, a recurring theme here is that ACS is often related to the need for and extent of rapid volume resuscitation. This can likely be attributed to splanchnic reperfusion following massive resuscitation.
- This is a somewhat more visual representation of the effects outlined in the previous slide.
- The performance of damage control surgery and recognition of abdominal compartment syndrome have dramatically improved patient survival, but at the cost of an open abdomen. Several management points deserve attention. Despite having a widely open abdomen, patients can develop recurrent abdominal compartment syndrome, which increases their morbidity and mortality; therefore, bladder pressure should be monitored every 4 hours, with significant increases in pressures alerting the clinician to the possible need for repeat operative decompression. Patients with an open abdomen lose between 500 and 2500 mL per day of abdominal effluent. Appropriate volume compensation for this albumin-rich fluid remains controversial, with regard to both the amount administered (replacement based on clinical indices vs. routine ½ mL replacement for every milliliter lost) as well as the type of replacement (crystalloid vs. colloid).
- The authors’ sequential closure technique for the open abdomen. A. Multiple white sponges (solid arrow), stapled together, are placed on top of the bowel underneath the fascia. Interrupted No. 1 polydioxanone sutures are placed approximately 5 cm apart (dashed arrow), which puts the fascia under moderate tension over the white sponge. B. After the sticky clear plastic vacuum-assisted closure (VAC) dressing is placed over the white sponges and adjacent 5 cm of skin, the central portion is removed by cutting along the wound edges. C and D. Black VAC sponges are placed on top of the white sponges and plastic-protected skin with standard occlusive dressing and suction. E. On return to the operating room (OR) 48 hours later, fascial sutures are placed from both the superior and inferior directions until tension precludes further closure; skin is closed over the fascial closure with skin staples. F. White sponges (fewer in number) are again applied and fascial retention sutures are placed with planned return to the OR in 48 hours.