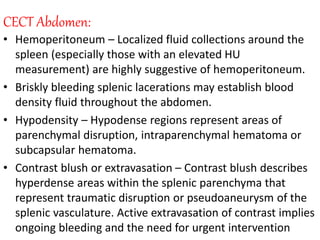
This document provides an overview of splenic injuries, including epidemiology, anatomy, evaluation, management, and guidelines. Key points include:
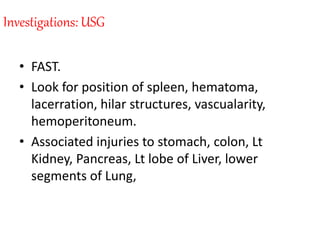
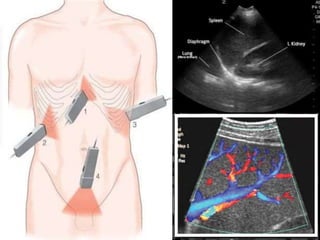
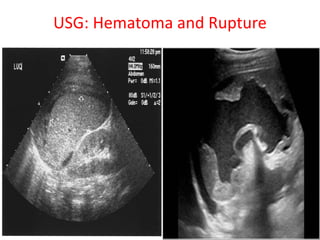
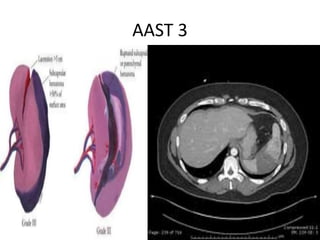
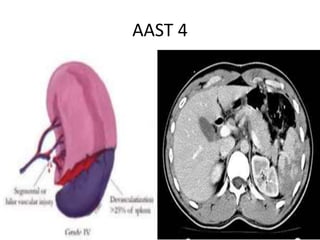
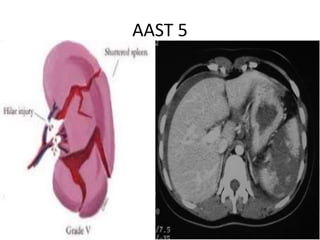
- The spleen is the most commonly injured organ in blunt abdominal trauma. Evaluation involves clinical exam, hematology tests, ultrasound, and CT scan to grade injuries.
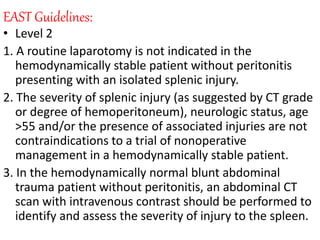
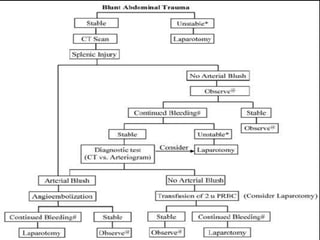
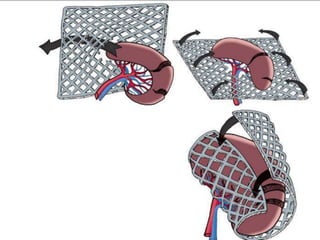
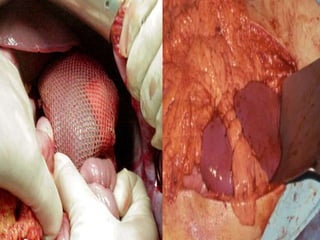
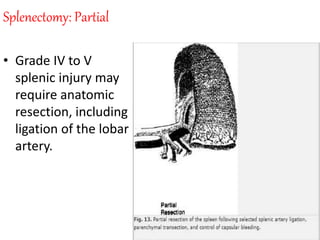
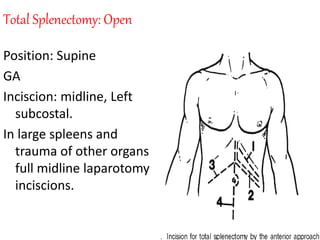
- Management depends on hemodynamic stability and injury grade. Options include non-operative management with observation or angioembolization, or splenectomy/splenorrhaphy during surgery.
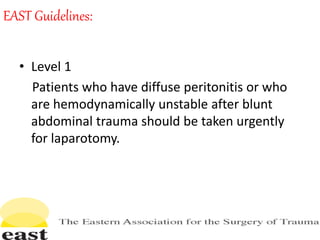
- Complications of splenic injuries and splenectomy include hemorrhage, infection, and post-splenectomy sepsis. Guidelines recommend attempting non-operative management for stable patients



![• Other organisms include: streptococcus
species, salmonella, Capnocytophaga
canimorous, Babesiosis.
High risk:
• children<5yrs old/>50 yrs,
• Splenectomy for Haemoglobiniopathies
[Thalasemeia, sickle cell a], Myelodysplasia,
malignancies.](https://image.slidesharecdn.com/splenicinjuriespptbymanjusb-180202175410/85/Splenic-injuries-ppt-by-manjusb-70-320.jpg)
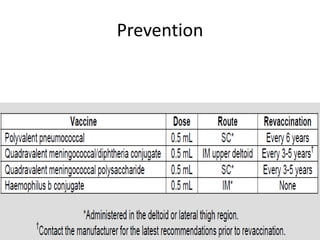
![Prevention:
Immunoprophylaxis:
• Vaccines aganst Strepto Pneumoniae [PPV23], H.Infl [H
influenza type B], Meningococcus
• Elective: At least 2 wks prior
• Emergency: PPV 23 immediate post op & Other two 2 wks
after surgery.
• [All 3 delayed for at least 2wks; because transient immune
suppression post op]
Antibody titre:
• No correlation between ab titre & clinical immunity
• Only in about 50% cases protective levels abs formed against
pneumococci
• Revaccination: CDC [united statescommunicable disese
control & prevention] to be revaccinated ppv 232-6 yrs after
splencetomy.](https://image.slidesharecdn.com/splenicinjuriespptbymanjusb-180202175410/85/Splenic-injuries-ppt-by-manjusb-71-320.jpg)