This document provides information about hernias, including:
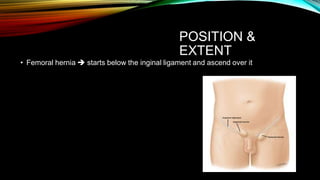
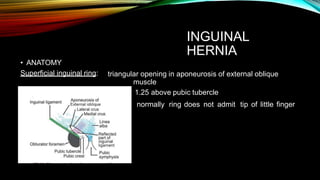
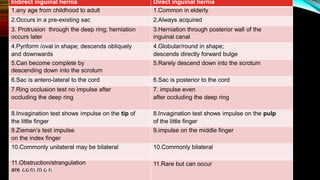
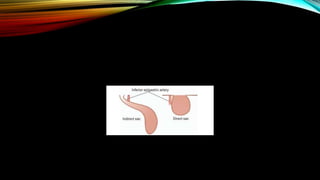
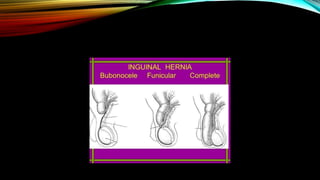
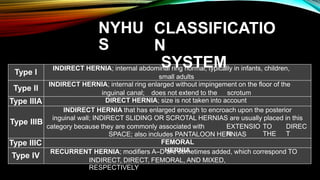
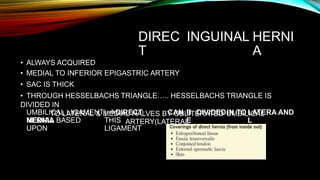
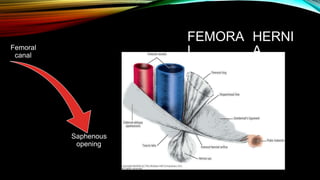
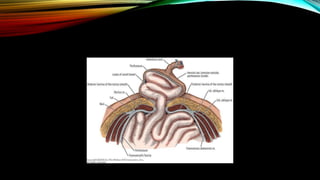
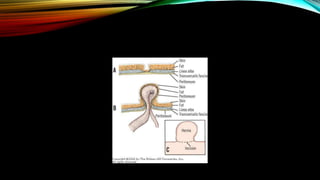
- It defines hernia and lists common types such as inguinal, femoral, umbilical etc.
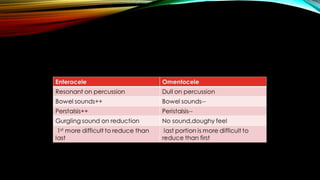
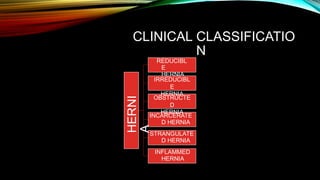
- It describes presenting complaints such as swelling and pain and signs of complications.
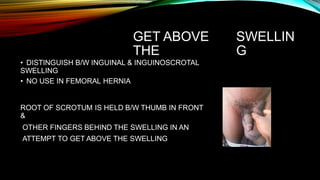
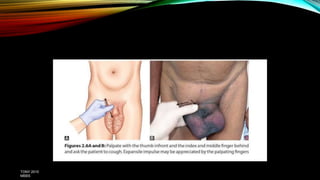
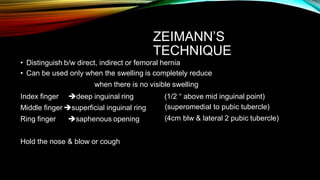
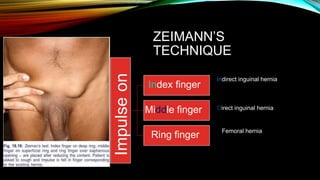
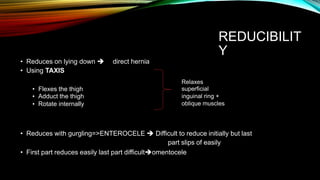
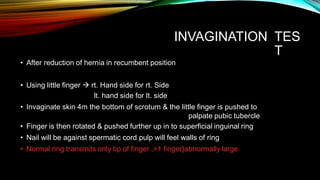
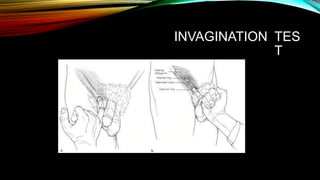
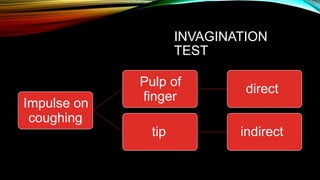
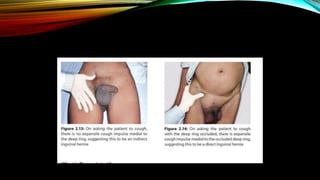
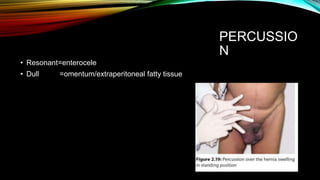
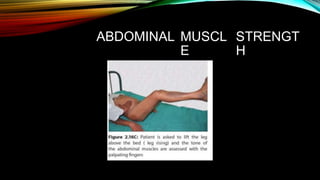
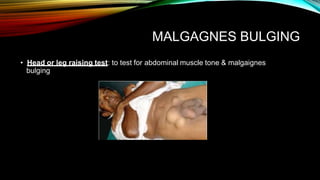
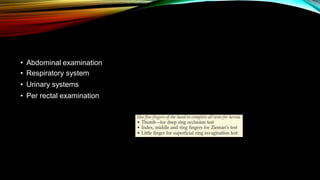
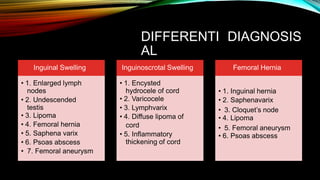
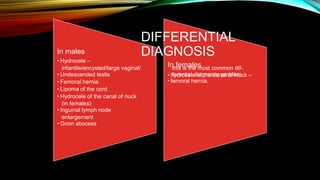
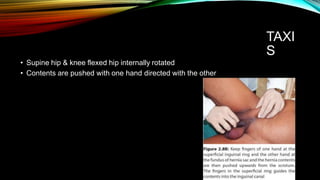
- It outlines the process for examining a patient with a hernia including inspection, palpation, reducibility tests and differential diagnosis.
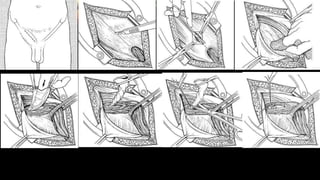
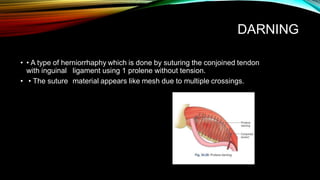
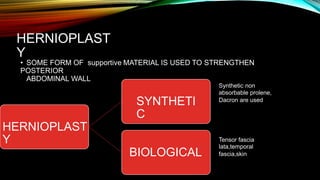
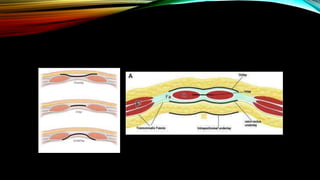
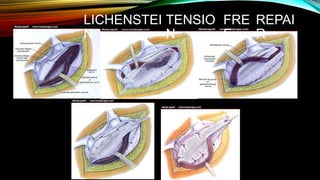
- It lists relevant investigations and discusses conservative and surgical treatment options for hernia repair.