Downloaded 94 times


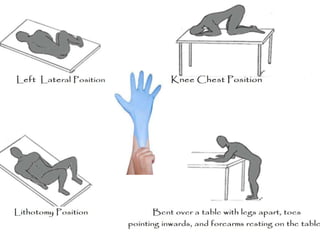

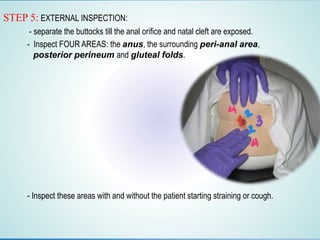

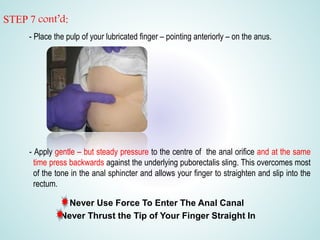
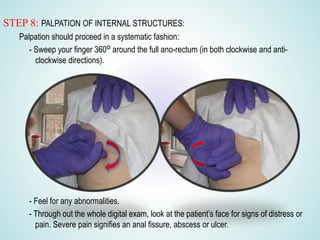
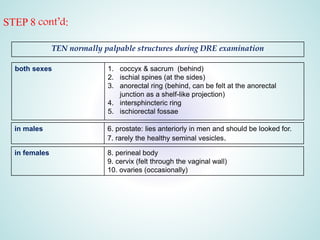
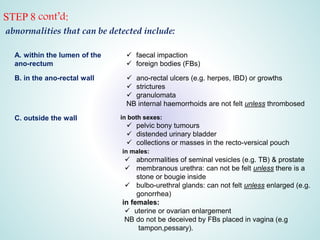
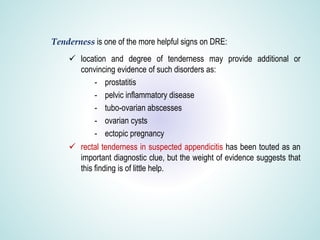
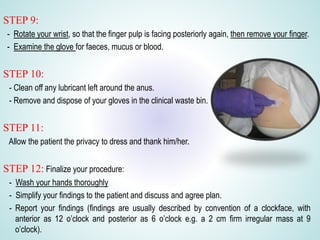


Digital Rectal Examination (DRE) is an important procedure in surgical practice used to examine the rectum and surrounding structures. It involves visual inspection of the external anal area and digital palpation of the internal rectum. The 12 key steps of a DRE are outlined, including introducing the procedure to the patient, inspecting externally, lubricating the finger, inserting the finger to palpate internal structures, and communicating findings to the patient. DRE allows examination of the prostate, cervix, and other pelvic structures to detect abnormalities like masses, hemorrhoids, or tenderness that can indicate various diseases.