Bladder tumors, specifically bladder cancer, occur when abnormal cells grow uncontrollably in the bladder lining, forming a tumor. These tumors can be non-muscle invasive (staying within the bladder lining) or muscle-invasive (penetrating into the bladder muscle). The most common type of bladder cancer is urothelial carcinoma.
Key Points:
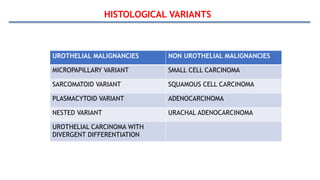
Types of Bladder Tumors:
The most common type is urothelial carcinoma, followed by squamous cell carcinoma and adenocarcinoma





















![Bladder Cancer NMIBC [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/non-muscleinvasivebladdertumoredmond-140716212950-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


















































