Downloaded 40 times







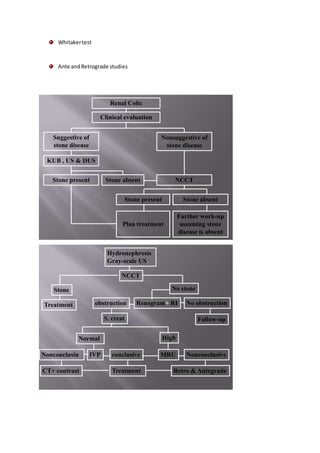

This document discusses obstructive uropathy, including its definitions, clinical presentation, pathophysiology, clinical implications, and diagnostic evaluation. Obstructive uropathy is resistance to urine flow along the urinary tract that can damage the kidneys. It may present with a wide range of symptoms depending on factors like degree and duration of obstruction. Diagnostic tests include intravenous pyelogram, renal ultrasound, renogram, CT, and MRI to identify the level and severity of obstruction and determine appropriate management.
























































































