Downloaded 13 times

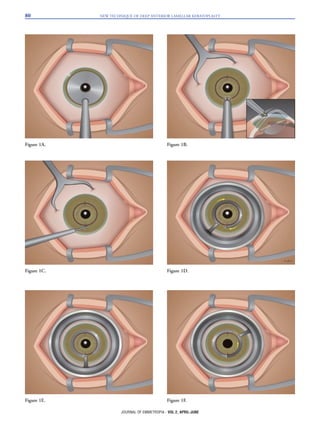
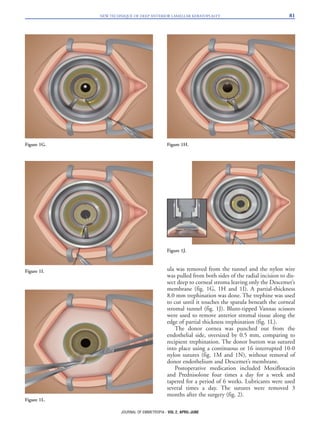



The document presents a new technique for deep anterior lamellar keratoplasty (DALK) aimed at improving corneal replacement by preserving the host's endothelial layer, especially beneficial for keratoconus patients. It describes a surgical procedure using a combination of a diamond knife and a nylon wire to create a smooth separation of the corneal stroma from Descemet's membrane, overcoming limitations of early DALK methods. This innovative technique offers a shorter learning curve for surgeons and aims to ensure better visual outcomes with fewer complications compared to traditional methods.





























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



