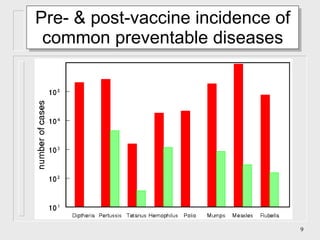
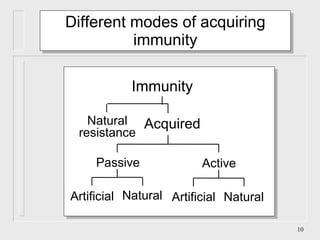
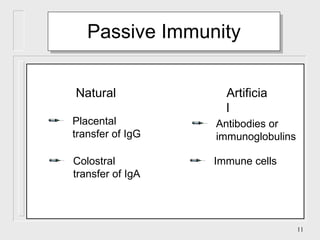
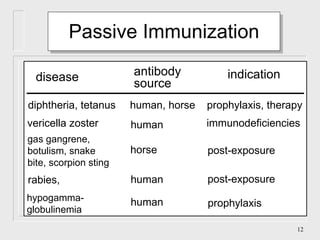
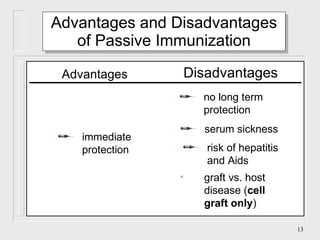
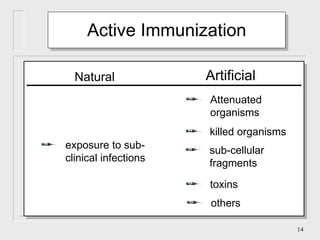
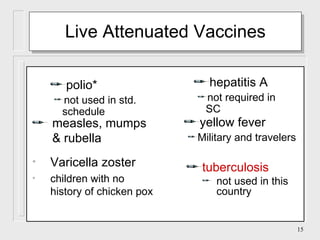
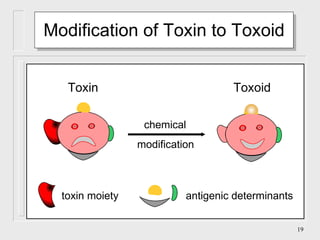
The document discusses the history and development of immunization and vaccines. It covers milestones such as variolation in ancient times, Jenner's discovery of the smallpox vaccine in 1780, and the development of vaccines for diseases like diphtheria, tetanus, pertussis, and polio between the 1920s-1960s. It also describes different types of immunity, vaccines, and potential adverse effects of vaccination.