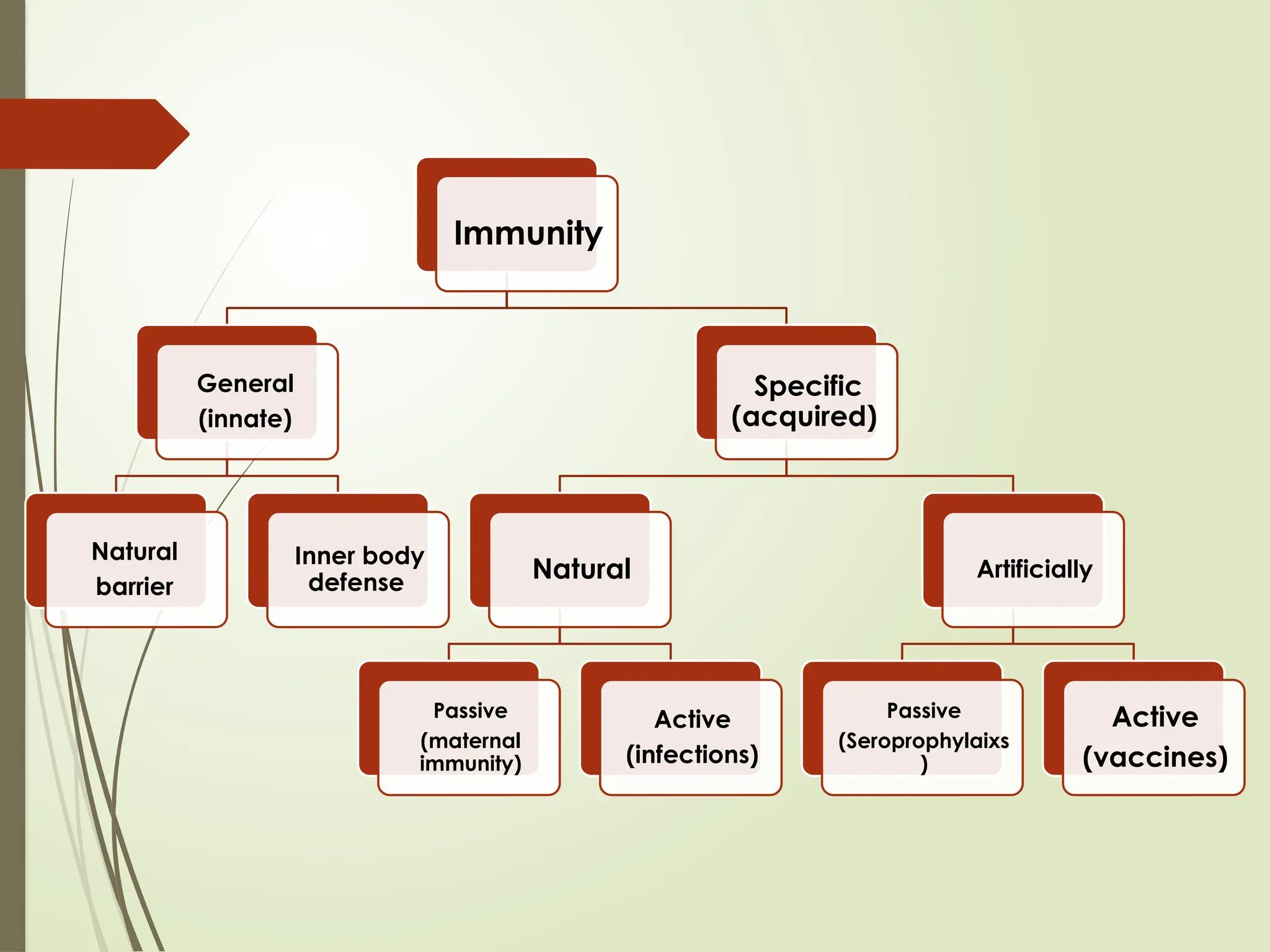
Specific (Acquired) Immunity
NaturallyAcquired immunity
Active natural acquired immunity :
Subclinical infection:
Repeated attacks immunity.
Clinical infection: One attack of infection different
degrees of immunity:
Absolute immunity as in yellow fever.
Solid or long lasting immunity e.g. measles, mumps,
chicken pox.
Mild or short lived immunity e.g. influenza.
Latent (persistence of dormant focus) infection
infection immunity (premunition) e.g. T.B.
8.
Specific (Acquired) Immunity
NaturallyAcquired immunity:
Passive natural acquired immunity :
Transplacental materno- foetal immunity : (in the
last weeks of pregnancy).
IGg small molecules can cross the placenta .
Give temporary immunity for 6-9 months. MMR
No maternal acquired immunity for pertussis (IgM) or T.B
(cell mediated immunity).
Colostrum & breast milk which contain:
High contents of antibodies (IgA).
Lysozyme & macrophages.
Passive artificially induced
immunity(Seroprophylaxis)
Definition: Passive artificially acquired immunity, induced by
injection of already formed immunoglobulin, antibodies, and
antitoxins, and lymphocytes to induce humoral or cellular immunity.
Advantages and disadvantages:
Give rapid but temporary protection without sensitization of
memory cells.
Used in prophylaxis or in treatment and before or after
exposure to infection.
Preparations:
Human preparations
Animal preparations
11.
Human preparations
1. Normalhuman immunoglobulins (NHI):
Prepared from large pool of plasma of volunteers in endemic area.
Used in prevention of measles, polio, rubella, virus hepatitis A.
Used for sero- prevention if given on early exposure and sero-
attenuation on late exposure e.g. measles, HBV.
2. Specific human immunoglobulins (SHI):
Prepared from plasma of actively immunized donors or
convalescent carriers of specific infections.
Used in prevention of viral disease as HBV, varicella zoster
infection and rabies.
Advantages:
Used in small doses, gives immediate immunity for long period (30-
50 days) Safe (does not lead to serum sickness or anaphylactic
reactions).
Disadvantages:
relatively expensive & not constantly available.
12.
Animal preparations
Anti-toxins: e.g.in seroprphylaxis or serotherapy
in Diphtheria, tetanus and gas gangrene
Given in large dose, give short protection (1-2 weeks).
May lead to severe hypersensitivity reaction (serum
sickness).
13.
Active artificially acquiredimmunity:
(Vaccines & Toxoids)
Vaccine
Definition : They are preparations of one or
more types of organisms
14.
Types of vaccines:
Live attenuated vaccines:
More potent than killed vaccines.
Given for only one dose except for polio (sabin).
Should not be given to pregnant women or persons
with immunodeficiency disease.
Examples:
Measles, mumps, rubella (or MMR),
sabin (OPV),
BCG (T.B),
yellow fever vaccine,
otten vaccine of plague.
15.
Types of vaccines:
Killed or in activated vaccines:
Killed by heat or chemicals .
Require primary series of 2-3 doses and some time
booster dose.
Given usually by intramuscular or subcutaneous
injection .
Examples :
Pertussis vaccine,
DPT,
salk of polio,
TAB of typhoid.
16.
Types of vaccines:
Polysaccharide (capsular) vaccine:
Examples :
Meningiococcal vaccine of meningitis.
Pneumococcal vaccine.
Haemophilus influenza type b vaccine.
Typhoid vaccine.
17.
Types of vaccines:
Surface antigen vaccines:
e.g. vaccine for viral hepatitis B manufactured
by genetic engineering in the yeast cells.
Recombinant vaccine
18.
Toxoid
Definition: detoxifiedtoxin so as to remove its
toxicity but still regain its antigenicity.
Examples : Diphtheria Toxoid & Tetanus Toxoid.
19.
System of activeimmunization:
1- Primary dose:
Single dose only e.g. MMR, measles, mumps, rubella,
BCG, yellow fever.
Multiple doses : e.g. DPT, OPV, HBV, TAB, koll's.
2- Booster dose: given after suitable period of time to
individual or group at risk to maintain satisfactory level of
immunity.
20.
Route of administrationof
vaccines & toxoid
S.C or IM for most immunizations.
ID (intradermal) BCG vaccine of T.B.
Orally sabin vaccine of polio (oral drops), oral
BCG vaccine.
Intranasal vaccine for influenza.
21.
Protective period ofactive
immunization:
Months e.g. cholera vaccine for 6 ms.
2 years e.g. TAB vaccine for typhoid (enterica).
3-5 years e.g. DPT, TT.
5 years e.g. BCG vaccine.
10 years e.g. yellow fever vaccine.
Solid (life long) immunity e.g. measles, mumps,
rubella, MMR.
22.
Effectiveness of active
immunization(protective value):
Absolute protective yellow fever.
Almost absolute (solid) 99% e.g. MMR, small
pox vaccine, toxoid of diphtheria & tetanus, HBV
(96%).
Highly protective 80- 90 % e.g BCG, pertussis,
polio.
Moderately protective 40- 60% e.g TAB,
cholera vaccine.
23.
Complications of activeimmunization
(Hazards or side effects):
General reaction: as fever, malaise, headache,
body aches.
Local reaction: pain, swelling, redness,
tenderness, abecess.
General infection: due to contaminated syringes
e.g HIV, HBV, HCV.
Specific hazards:
BCG if given S.C or IM.
Rabies vaccine especially new tissue vaccine.
Pertussis vaccine encephalopathy.







































![]]]العادات غير السوية في الصحة النفسية.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/random-250209164454-484d3b90-thumbnail.jpg?width=640&height=640&fit=bounds)





























