
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Macular cherry red spot
Similar to Macular cherry red spot (20)
More from SIDESH HENDAVITHARANA
Recently uploaded
Recently uploaded (20)
Macular cherry red spot
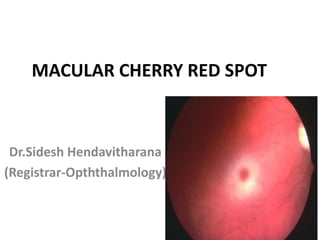
- 1. MACULAR CHERRY RED SPOT Dr.Sidesh Hendavitharana (Registrar-Opththalmology)
- 2. . Pt with macular cherry red spot Sudden visual loss Spontaneous Dilated retinal examination FFA Diffuse edema CRAO Central retinal defect Macular hole Blunt ocular trauma Dilated funduscopy Central retinal haemorrhage Berlin’s edema Congenital condition Consider: Niemann-pick disease Tay-sachs disease Sandhoff’s disease Generalized gangliosidoses Immunosupression Consider:PORN/ ARN
- 3. CENTRAL RETINAL ARTERY OCCLUSION • Symptoms – Sudden profound vision loss,painless except GCA – VA severely reduced.Absence of LP usually indicates either GCA or ophthalmic artery occlusion. – RAPD is profound,sometimes total(amaurotic pupil)
- 4. funduscopy Attenuation of arteries and veins with sludging and segmentation of blood column (cattle trucking/boxcarring) Cloudy edematous retina Cherry red spot(orange reflex from intact choroid strands out at the thin foveola,in contrast to the surrounding pale retina) Peripapillary retina may be swollen and opaque. Over a few days to weeks the retinal cloudiness and cherry red spot gradually dissapear. Late signs include optic atropy,vessel sheathing and patchy inner retinal atrophy,vessel sheathing and patchy inner retinal atrophy and RPE changes. About 2% of eyes with CRAO develop retinal or disc neovascularization Rubeosis iris may occur in up to about 1 in 5 eyes.
- 5. . • .
- 6. . • .
- 7. . • .
- 8. Investigation • OCT – Highly reflective embolic plaque within the superficial optic nerve head. • FA – Variable delay in arterial filling and masking of background choroidal flourescence by retinal edema. • Electroretinography – Diminished b-wave is present Review 4wkly interval to detect incipient neovascularization.In this event,PRP should be considered and anti VEGF might also be considered. Appropriate systemic management is critical.
- 9. Metabolic storage disease • Rare metabolic diseases,often enzyme deficiencies,leads to the pathological accumulation of lipid based material in various tissues. • With the passage of time the spot become less evident due to retinal nerve fibre layer degeneration,and consecutive optic atrophy is seen. • They are almost exclusively AR.
- 10. GM1-gangliosidosis(generalized) Inheritance-AR Defect-deficiency of beta galactosidase 1 Systemic features-coarse facies,stiff joints,growth deficiency and severe cerebral degeneration leading to death by the age of 2 yrs. ocular features-macular cherry red spot in 50% of cases and very subtle corneal clouding.
- 11. Mucolipidosis • Inheritance-AR • Systemic • Late-onset – (after the age of 7 yrs)with myoclonus and seizures,compatible with normal life span • Severe – Starts before the age of 2 yrs and is characterized by severe neurodegeneration hurler-like facies,hepatoplenomegaly,deafness and death in early childhood. • Ocular features – Include corneal clouding,macular cherry red spot,optic atrophy and occasionaly punctate lens opacities.
- 12. GM2-gangliosidosis • Tay-sachs disease – Inheritance-AR – Pathogenesis – Deficiency of hexosaminidase A leads to accumulation of ganglioside in the brain and retina – Systemic features – Progressive neurological deterioration starting within 6 months or birth with death by 2 yrs. • Sandhoff disease – Inheritance-AR – Pathogenesis • Hexosaminidase A and B deficiency – Systemic features • Neurological degeneration similar to Tay-sach disease – Ocular features • Macular cherry-red spot and early-onset blindness.
- 13. Niemann-Pick disease • Main types- A to C • Types A (acute neuronopathic) – Inheritance-AR – Systemic feature – Present in infancy and are characterized by severe psychomotor deterioration,massive hepatosplenomegaly and death by the 4th year. – Ocular features are macualr cherry-red spot in 50% and subtle corneal clouding. • Type B(chronic non-neuronopathic) – Inheritance-AR – Systemic features – Present in the teenage years or early adulthood and are characterized by hepatosplenomegaly,and involvement of the lung and bone marrow. – CNS disease does not occur and survival upto 20 yrs after presentation is possible. – Ocular disease – Cherry red spot at macula and bull’s eye maculopathy.
- 14. Farber disease • Inheritance-AR • Pathogenesis – Lysosomal storage disease due to defective ceramidase • Systemic features – Include hoarseness,aphonia,dermatitis, lymphadenopathy,psychomotor retardation and renal and cardiopulmonary disease • Ocular features – Include macular cherry red spot,pingueculum-like conjunctival lesions and nodular corneal opacity
- 15. Caucasian child with a cherry “red” spot Tay-Sachs disease Canadian aboriginal child with a cherry “brown” spot Sandhoff disease East Indian child with a cherry “black” spot Sandhoff disease
- 16. Progressive retinal necrosis • Devastating necrotizing retinitis,usually caused by VZV and other herpes viruses • May be associated with immunocompromised states. • Ocular features • Rapidly progressive unilateral or bilateral visual loss. • Ant.uveitis and vitritis are minimal,in contrast to CMV retinitis and ARN. • RETINITIS:3 Stages recognized. 1) Early:multifocal yellow white deep retinal infiltrates.The macula may be involved in early stage,often giving a cherry red spot. 2) Established/middle:The signs typically spread rapidly around the retina,with extansive full thickness necrosis.signs of vasculitis are absent or mild,and significant h’age is uncommon. 3) Late:scarring is plaque like and characterized as ‘cracked mud’.RRD is very common,as in optic atrophy. • Investigation: • Vitrious/aqueous PCR for viral DNA • TREATMENT – Immune rescue with HAART together with aggressive antiviral therapy – VR surgery for RD
- 17. ACUTE RETINAL NECROSIS – Rare but devastating necrotizing retinitis. – It typically affects otherwise healthy individuals,but tend to be caused by HSV in younger and VZV in older pts,other herpes viruses are suspected. – Prognosis is relatively poor • Systemic features: – ARN has been reported following and occurring simultaneously with HSV encephalitis and herpetic skin infection
- 18. Ocular features • Initialy unilateral with blurred vision and floaters. • Pain is usually a feature. • This American uveitis society defines a criteria for diagnosis 1) Prominent anterior uveitis and vitritis(episcleritis and scleritis may occur) 2) One or more discrete foci of peripheral retinal necrosis. 3) Deep yellow-white infiltrate with well defined borders are seen. 4) Circumferential spread of retinal involvement .posterior pole involvement is late. 5) Occlusive retinal vasculitis including arteritis 6) Rapid progression of disease in the absence of treatment • Investigation – Vitrious/aqueous PCR for viral DNA • TREATMENT – Intravenous acyclovir/oral valacyclovir or famcyclovir/intravitreal gancyclovir or foscarnet – Vitrectomy/Laser retinopexy for RRD
- 19. Thank you