Downloaded 102 times


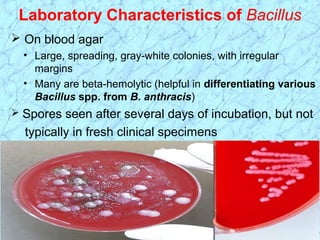



























This document discusses spore-forming gram-positive rods including Bacillus and Clostridium species. Key points include: - Bacillus and Clostridium are spore-forming, gram-positive rods that can be aerobic or anaerobic. Important medically are B. anthracis, B. cereus, C. botulinum, C. tetani, C. perfringens, and C. difficile. - Laboratory diagnosis involves culturing on blood agar and observing colony morphology, hemolytic patterns, and microscopic appearance including spore formation. Serological and molecular tests can also identify toxins. - Major diseases include anthrax, botulism,



































































































