Clostridium are Gram-positive, obligate anaerobic, spore-forming bacteria that can cause disease. There are over 100 Clostridium species including pathogens that cause gas gangrene (C. perfringens), tetanus (C. tetani), botulism (C. botulinum), pseudomembranous colitis (C. difficile). Clostridium species are rod-shaped and can form spores to protect themselves in harsh environments. The spores vary in shape and position between species and can be used to identify Clostridia. Several Clostridium species produce potent toxins that are the main virulence factors and cause of disease.
These bacteria make spores, which act like protective coatings that help the bacteria survive. Under certain conditions, such as when food is kept at an unsafe temperature (between 40°F–140°F), C. perfringens can grow and multiply. After someone swallows the bacteria, it can produce a toxin (poison) that causes diarrhea.
Common sources of C. perfringens infection include meat, poultry, gravies, and other foods cooked in large batches and held at an unsafe temperature. Outbreaks tend to happen in places that serve large groups of people, such as hospitals, school cafeterias, prisons, and nursing homes, and at events with catered food. C. perfringens outbreaks occur most often in November and December. Many of these outbreaks have been linked to foods commonly served during the holidays, such as turkey and roast beef.
Anyone can get food poisoning from C. perfringens. Young children and older adults are at higher risk for severe illness.
Toxoplasmosis is considered one of the neglected parasitic infections of the United States, a group of five parasitic diseases that have been targeted by CDC for public health action.Q fever is a disease caused by the bacteria Coxiella burnetii. This bacteria naturally infects some animals, such as goats, sheep, and cattle. C. burnetii bacteria are found in the birth products (i.e. placenta, amniotic fluid), urine, feces, and milk of infected animals.
These bacteria make spores, which act like protective coatings that help the bacteria survive. Under certain conditions, such as when food is kept at an unsafe temperature (between 40°F–140°F), C. perfringens can grow and multiply. After someone swallows the bacteria, it can produce a toxin (poison) that causes diarrhea.
Common sources of C. perfringens infection include meat, poultry, gravies, and other foods cooked in large batches and held at an unsafe temperature. Outbreaks tend to happen in places that serve large groups of people, such as hospitals, school cafeterias, prisons, and nursing homes, and at events with catered food. C. perfringens outbreaks occur most often in November and December. Many of these outbreaks have been linked to foods commonly served during the holidays, such as turkey and roast beef.
Anyone can get food poisoning from C. perfringens. Young children and older adults are at higher risk for severe illness.
Toxoplasmosis is considered one of the neglected parasitic infections of the United States, a group of five parasitic diseases that have been targeted by CDC for public health action.Q fever is a disease caused by the bacteria Coxiella burnetii. This bacteria naturally infects some animals, such as goats, sheep, and cattle. C. burnetii bacteria are found in the birth products (i.e. placenta, amniotic fluid), urine, feces, and milk of infected animals.
Cryptosporidium exhibits a monoxenous lifecycle and affects both humans and animals. Infected domestic animals are reservoirs for susceptible humans. in the lifecycle of the cryptosporidium, Thin-wall oocyst (used for autoinfection) and Thick wall oocyst are (thrown into the environment for infecting another host). Invaginate cell membrane and forming #bi-layered membranous vacuole (parasitophorous vacuolar membrane) creates a conducive environment for the parasite for escaping the host immune system.
Cryptosporidium exhibits a monoxenous lifecycle and affects both humans and animals. Infected domestic animals are reservoirs for susceptible humans. in the lifecycle of the cryptosporidium, Thin-wall oocyst (used for autoinfection) and Thick wall oocyst are (thrown into the environment for infecting another host). Invaginate cell membrane and forming #bi-layered membranous vacuole (parasitophorous vacuolar membrane) creates a conducive environment for the parasite for escaping the host immune system.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
1. Clostridium
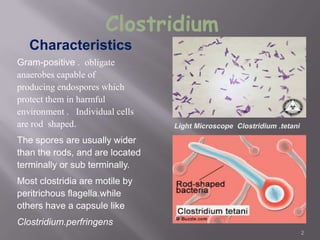
Gram-positive . obligate
anaerobes capable of
producing endospores which
protect them in harmful
environment . Individual cells
are rod shaped.
The spores are usually wider
than the rods, and are located
terminally or sub terminally.
Most clostridia are motile by
peritrichous flagella.while
others have a capsule like
Clostridium.perfringens
Characteristics
2
2.
Clostridium consists of around 100 species that
include common free-living bacteria as well as
important pathogens There are five main
species
responsible for disease in
humans.
C. perfringens: gas gangrene; food poisoning
C. tetani: tetanus
C. botulinum: botulism
C. difficile: pseudomembranous colitis
C.Sordellii : can cause a fatal infection in exceptionally rare
cases after medical abortions
3. The shape an position of spores varies in different
species and is useful the identification of
Clostridia
*Central in Cl.bifermentans
*Sub terminal in Cl.perfringens
*Oval or terminal in Cl.tertium
*Spherical and terminal giving
drum stick appearance in Cl.tetani
4
4. C. perfringens is a
relatively large Gram-
positive short fat
bacilli with blunt ends.
It is capsulate and
non-motile. Anaerobic.
It grows quickly on
laboratory media on
blood agar ( B –
Haemolytic )
5
5. Liquid medium for
cultivation cooked
meat broth
Thiglyclolate broth
CMB contain
unsaturated fatty
acids which take up
oxygen
6
7.
It distinguish between different
species of bacteria.
The lactose (milk
sugar), litmus (pH indicator),
and casein(milk protein)
contained within the medium can
all be metabolized by different
types of bacteria.
Milk is the first substrate used to
maintain bacteria, this test allows
for accurate depiction of bacterial
types. The addition of litmus,
other than explaining the pH type,
acts as an oxidation-reduction
indicator. The test itself tells
whether the bacterium can
ferment lactose, reduce litmus,
form clots, form gas,
8. This test is done to detect the lecithinase
activity
The M.O is streaked on the medium containing egg
yolk (contains lecithin)
The plate is incubated anaerobically at 37 C for 24 h
Colonies of Cl. perfringens are surrounded by zones
of turbidity due to lecithinase activity and the effect is
specifically inhibited if Cl. perfringens antiserum
containing antitoxin is present on the medium
`
9
9. C. perfringens Nagler Reaction
NOTE: Lecithinase (α-toxin; phospholipase) hydrolyzes
phospholipids in egg-yolk agar around streak on right.
Antibody against α-toxin inhibits activity around left streak.
10
13. The organisms
associated with gas
gangrene attack soft
tissues by producing
toxins and aggressins,
and some strains of
the bacteria produce
enterotoxins and
cause food poisoning
14
14. If there are pieces of necrotic tissue in
the wound, small pieces should be
transferred aseptically into a sterile
screw-capped bottle and examined
immediately by microscopy and culture.
Specimens of exudate should be taken
from the deeper areas of the wound
where the infection seems to be most
pronounced.
15
16. Clostridium tetani
Anaerobic bacteria of the genus species Clostridium it is gram
positive, slender bacillus and it has spherical terminal spores
giving drum stick appearance
It is non capsulated & motile with peritrichus flagella
It produces a potent biological toxin, tetanospasmin, and is the
causative agent of tetanus a disease characterized by painful
muscular spasms that can lead to respiratory failure and, in up
to 40% of cases, death.
17. An infectious disease caused by
contamination of wounds from the
bacteria Clostridium tetani, or the
spores they produce that live in the soil,
and animal feces
Infection follows when spores
become activated and develop
into gram-positive bacteria that multiply
and produce a very powerful toxin
(tetanospasmin) that affects the
muscles.
18. Tetanus spores are found throughout the
environment, usually in soil, dust, and animal waste.
Tetanus is acquired through contact with the
environment; it is not transmitted from person to
person.
19. The usual locations for the bacteria to enter the
body:
Puncture wounds (such as those caused by rusty
nails, splinters, or insect bites.)
Burns, any break in the skin, and IV drug access sites are
also potential entryways for the bacteria.
20.
1. It inhibits the release of acetylcholine thus it
interferes with neuromuscular transmission.
2. Inhibition of postsynaptic spinal neurons by
blocking the release of an inhibiting mediator
21. Gram +ve stains grow on blood agar media
aerobically
Inoculation of culture in to 2 mice one is protected
with anti-toxin and the other is unprotected (dies with
typical tetanic spasms )
22.
"C. diff", is a species
positive
-
Gram
of
of the genus
bacteria
that
Clostridium
causes diarrhea and
other intestinal
disease when
competing bacteria
are wiped out by
antibiotics.
23.
Most common cause of nosocomial diarrhea.
Rate and severity of C. difficile-associated diarrhea
(CDAD) increasing.
Clostridium difficile is a bacterium that can cause
symptoms ranging from diarrhea to life-threatening
inflammation of the colon. Illness from C. difficile
most commonly affects older adults in hospitals or
in long term care facilities and typically occurs after
use of antibiotic medication
25.
C. difficile bacteria can be found throughout the
environment — in soil, air, water, and human
and animal feces. A small number of healthy
people naturally carry the bacteria in their large
intestine. But C. difficile is most common in
hospitals and other health care facilities, where
a much higher percentage of people carry the
bacteria.
26. Reservoir
Infectious Agent
C.difficile
Means of
Transmission
Portal of entry
Susceptible Host
Chainof infection
Bowel and
Contaminated
environment
Contact
transmission from
contaminated
hands,
equipment or the
environment
Faecal/Oral
>65 years
History of antibiotic use
Recent received
healthcare
Underlying conditions
Abdominal surgery
Weakened immunity
27.
Disruption of normal
colonic flora
Colonisation with C.
difficile
Production of toxin A
+/- B
Mucosal injury and
inflammation
28.
Toxigenic strains
produce 2 major
toxins:
toxin A
(enterotoxin)
toxin B (cytotoxin)
Neutralised by C.
sordellii antitoxin
29.
Watery diarrhea three or more times a day for two
or more days
Mild abdominal cramping and tenderness
Watery diarrhea 10 to 15 times a day
Abdominal cramping and pain, which may be
severe
Fever
Blood or pus in the stool
Nausea
Dehydration
Loss of appetite
Weight loss
31. The Specimen
Fresh is best (test within 2 hours)
Liquid or loose, not solid
If unable to test within 2 hours, refrigerate
at 4 C for up to 3 days
Freeze at -70 C (not -20 C) if testing will
be delayed
Specimen quality will influence test results
42.
The symptoms of botulism are similar to
those of Guillain-Barré syndrome, stroke,
and myasthenia gravis.
As a result, botulism is probably
substantially under-diagnosed.
Serum electrolytes, renal and liver function
tests, complete blood tests, urinalysis, and
electrocardiograms will all be normal unless
secondary complications occur.
43.
The incubation period varies according to
the mode of transmission, rate of absorption
of the toxin, and the total amount and type
of toxin.
Foodborne botulism usually takes 24-36
hours to manifest itself.
Wound botulism often takes 3 or more days
to appear.
Inhalation botulism has occurred very rarely,
but incubation times may range from several
hours to perhaps days, again depending
upon the type and amount of toxin inhaled.
44.
All four types of botulism result in symmetric
descending flaccid paralysis of motor and
autonomic nerves always beginning with the
cranial nerves. These symptoms are
preceded by constipation in cases of infant
botulism.
Symptoms include:
Double or blurred vision
Drooping eyelids
Dry mouth
Difficulty Swallowing
Muscle weakness
45.
If left untreated symptoms may expand to
include paralysis of respiratory muscles as
well as the arms and legs.
Asphyxiation due to respiratory paralysis is
the most common cause of death in
botulism cases.
46.
Proper food preparation is one of the most
effective ways to limit the risk of exposure to
botulism toxin.
Boiling food or water for ten minutes can
eliminate some strains of Clostridium botulinum
as well as neutralize the toxin as well.
However, this will not assure 100% elimination.
Limiting growth of Clostridium botulinum and
the production of botulism toxin is an
alternative to their outright destruction.
47.
Now manufactured under the name ―Botox‖
Experimentally used for treating migraine
headaches, chronic low back pain, stroke,
cerebral palsy, and dystonias (neurologic
diseases involving abnormal muscle posture
and tension)
Frequent injections allows an individual to
develop antibodies
Studies carried out to determine feasibility of
other strains of BoNT
BoNT B manufactured for treatment of
cervical dystonia in 2000 as ―Myobloc‖