Cardiac Amyloidosis
•Download as PPTX, PDF•
18 likes•6,081 views

amyloid .cardiac amyloidosis. Pathogenetic steps in the development of amyloid diseases.AL amyloidosis. ATTR amyloidosis.ATTRwt amyloidosis. Potential for misdiagnosis of amyloidosis

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Cardiac Amyloidosis
Similar to Cardiac Amyloidosis (20)
More from magdy elmasry
More from magdy elmasry (20)
Recently uploaded
Recently uploaded (20)
Cardiac Amyloidosis
- 1. Magdy El-Masry Prof. of Cardiology Tanta University
- 2. Amyloid Rudolph Virchow in 1854 adopted the term “amyloid” to refer to tissue deposits of material that stained in a similar manner to cellulose when exposed to iodin Amyloid has blue staining with iodine . (Virchow 1854) Cellulose (amylum) has the same staining.
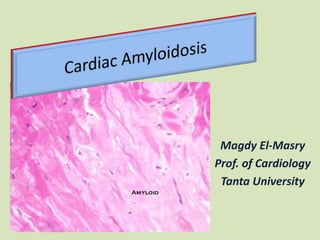
- 3. (a) H and E stain showing extensive amyloid infiltration of the myocardium (light pink) which distorts and separates the myocytes (darker pink). (b) Staining with Sulfated Alcian Blue (another patient) shows typical amyloid staining with turquoise staining of the amyloid and yellow myocyte staining.
- 4. The amyloidoses are a diverse group of disorders whose effects are felt in every part of the body and every corner of the globe. The hallmark of these diseases is the aggregation and deposition of misfolded protein as insoluble amyloid fibrils. Amyloidosis A protein misfolding disease
- 5. The two most common forms of cardiac amyloidosis are the AL and ATTR types. Pathogenetic steps in the development of amyloid diseases.
- 6. Inherited mutations in transthyretin cardiac amyloidosis (ATTR) or the aging process in wild-type disease (ATTRwt) cause destabilization of the transthyretin (TTR) protein into monomers or oligomers, which aggregate into amyloid fibrils. These insoluble fibrils accumulate in the myocardium and result in diastolic dysfunction, restrictive cardiomyopathy, and eventual congestive heart failure Pathogenetic steps in the development of amyloid diseases.
- 7. AL amyloidosis A : Amyloid fibril protein >>> derived from immunoglobulin light (L) chains ATTR amyloidosis A : Amyloid fibril protein >>> derived from the plasma protein transthyretin ( TTR ) ATTRwt amyloidosis Wild-type ATTR ATTR V30M amyloidosis Where the normal valine residue at position 30 has been substituted with methionine.
- 8. Some types of amyloid have a greater predilection for the heart than others. The two most common forms of cardiac amyloidosis are the AL and ATTR types. AL amyloidosis may involve almost any other organ in the body, whereas inherited ATTR amyloidosis variably involves the heart and autonomic and peripheral nerves. Nonhereditary ATTR amyloidosis has almost exclusively a cardiac phenotype. The commonly diagnosed types of cardiac amyloidosis
- 9. The commonly diagnosed types of cardiac amyloidosis Primary (AL) ATTRwt (Senile CA) ATTR V122I ATTR T60A ATTR V30M Precursor/ amyloidogenic protein Monoclonal Immuno- globulin light chain Wild-type transthyretin Variant transthyretin Variant transthyretin Variant transthyretin Average age at presentation 60–70 years 70–80 years ≥60 years ≥60 years 30–40 or 50– 60 years Common ethnicity Any Caucasian African/ Caribbean Caucasian (Irish Any (Portuguese, Swedish, Japanese
- 10. Primary (AL) ATTRwt (Senile CA) ATTR V122I ATTR T60A ATTR V30M Frequency of cardiac involvement 40–50% Almost 100% Almost 100% Detectable in at least 90% Uncommon Other systemic involvement Kidney, liver, soft tissue, nerves, spleen Carpal tunnel (bladder, spine) Carpal tunnel Nerves Nerves The commonly diagnosed types of cardiac amyloidosis AL, monoclonal immunoglobulin light chain amyloidosis; ATTR, transthyretin amyloidosis; ATTRwt; transthyretin amyloidosis associated with wild-type transthyretin; SCA, senile cardiac amyloidosis
- 11. Famous People with Amyloidosis
- 12. A constant complaint of patients with rare diseases is the long delay between the first symptom and the clinical diagnosis made by physicians. This is also true for amyloidosis and can be explained in part by the great number of organs and systems that can be affected by amyloid deposits leading to a large variety of symptoms, none of them being specific of the disease. Virtually all organs can be affected by amyloidosis. Clinical Diagnosis Amyloidosis as a Great Masquerader
- 13. Potential for misdiagnosis: physician- and disease related factors
- 15. Factors leading to misdiagnosis Fragmented knowledge among different specialties and subspecialties Shortage of centres and experts dedicated to specialised disease management Erroneous belief it is an untreatable disease Physician-related factors
- 16. Factors leading to misdiagnosis Common misconceptions about diagnosing and typing amyloid • Low voltage is not sensitive nor specific finding in isolation to exclude the presence of CA • Serum protein electrophoresis is not a sufficient screening test to exclude the presence of a plasma cell disorder that can cause AL amyloid • A fat pad biopsy has a sensitivity for AL amyloid of 70 % at best and is positive in<50 % of subjects with ATTR CA Physician-related factors
- 17. Factors leading to misdiagnosis Disease-related factors Rarity Intrinsic phenotypic heterogeneity Genotypic heterogeneity in ATTR Necessity of target organ tissue histological diagnosis in the vast majority of cases
- 18. Main known determinants of phenotypic heterogeneity in ATTR.
- 19. Genotype–phenotype correlation in ATTR. Some mutations are associated with both neurological and cardiac manifestations, whereas others lead to an exclusively neurological disease and a small number are associated with an exclusively cardiological phenotype.
- 20. Caveats and pearls in cardiac amyloidosis • A definite diagnosis of cardiac amyloidosis requires not only tissue biopsy proof of amyloidotic infiltration but also the identification of the precursor protein causing amyloid (since treatment strictly depends upon aetiology) • A high index of suspicion is mandatory for the recognition of CA in the clinical arena (e.g. if you don’t think of it, you won’t diagnose it!)
- 21. Caveats and pearls in cardiac amyloidosis • Cardiac amyloid should be suspected in any patient with heart failure, unexplained increased LV wall thickness and non-dilated LV • In a patient with an initial diagnosis of HCM, look for the infiltrative phenotype hidden beneath the hypertrophic one!
- 22. Caveats and pearls in cardiac amyloidosis • A distinctive sign of CA is the abnormal ratio between LV thickness and QRS voltages rather than low QRS voltages alone. The absence of low QRS voltages does not rule out a CA if the context is otherwise fitting and up to 20 % of subjects with CA can have ECG evidence of LV hypertrophy
- 23. Caveats and pearls in cardiac amyloidosis • In an elderly man with unexplained concentric LV hypertrophy, especially in the absence of hypertension, always consider the possibility of wild-type TTR CA! • CA in an elderly patient with monoclonal gammopathy is not necessarily related to AL: consider the possibility of wild-type TTR +MGUS (monoclonal gammopathy of uncertain significance)
- 24. Caveats and pearls in cardiac amyloidosis • Longitudinal LV function can be severely depressed despite a normal LV ejection fraction and the myocardial contraction fraction are often low suggesting reduced global myocardial shortening • Myocardial deformation is reduced in CA, but the apex is generally spared
- 25. Caveats and pearls in cardiac amyloidosis • In CA, LGE (late Gd enhancement ) distribution at MRI is heterogeneous: subendocardial LGE is not the only diagnostic pattern and the absence of LGE does not exclude CA • Bilateral carpal tunnel syndrome in a man with HCM- like phenotype on echo is highly suggestive of TTR- related CA
- 26. Evaluation to Diagnose ATTR Diagnostic pathway to arrive at a diagnosis of ATTR
- 27. Diagnostic pathway to arrive at a diagnosis of ATTR
- 30. Emerging Therapies for Transthyretin Cardiac Amyloidosis
- 31. Emerging Therapies for Transthyretin Cardiac Amyloidosis
- 32. References Rapezzi C et al . Cardiac amyloidosis: the great pretender. Heart Fail Rev 2015; 20:117–124 Patel K S & Hawkins P N . Cardiac amyloidosis: where are we today?. J Intern Med 2015; 278: 126–144. Castano A et al. Emerging Therapies for Transthyretin Cardiac Amyloidosis Could Herald a New Era for the Treatment of HFPEF. http://www.acc.org/latest-in- cardiology/articles/2015/10/13/08/35/emerging-therapies-for-transthyretin- cardiac-amyloidosis Gertz M A et al . Diagnosis, Prognosis, and Therapy of Transthyretin Amyloidosis. J Am Coll Cardiol. 2015;66(21):2451-2466