Downloaded 576 times
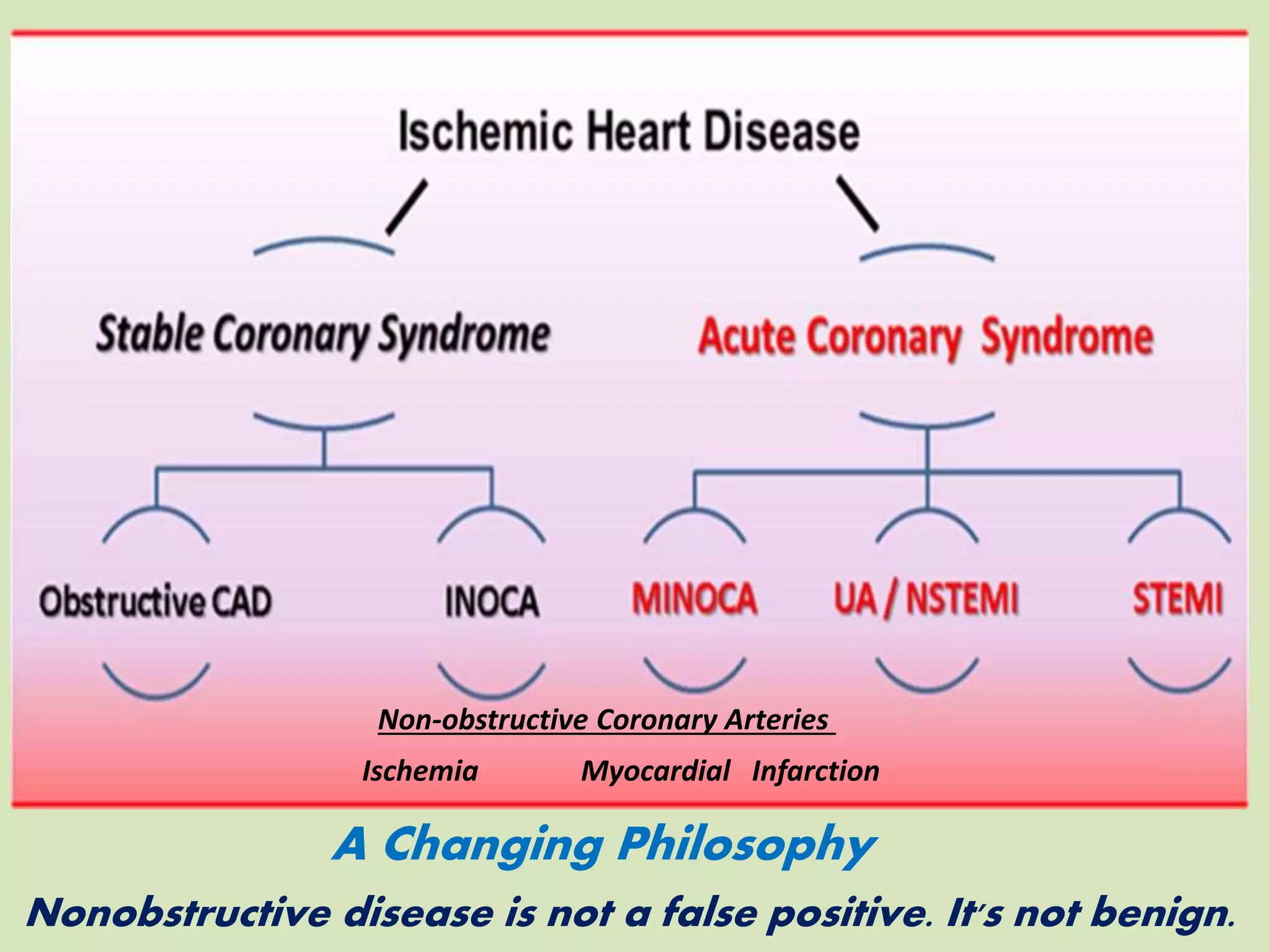
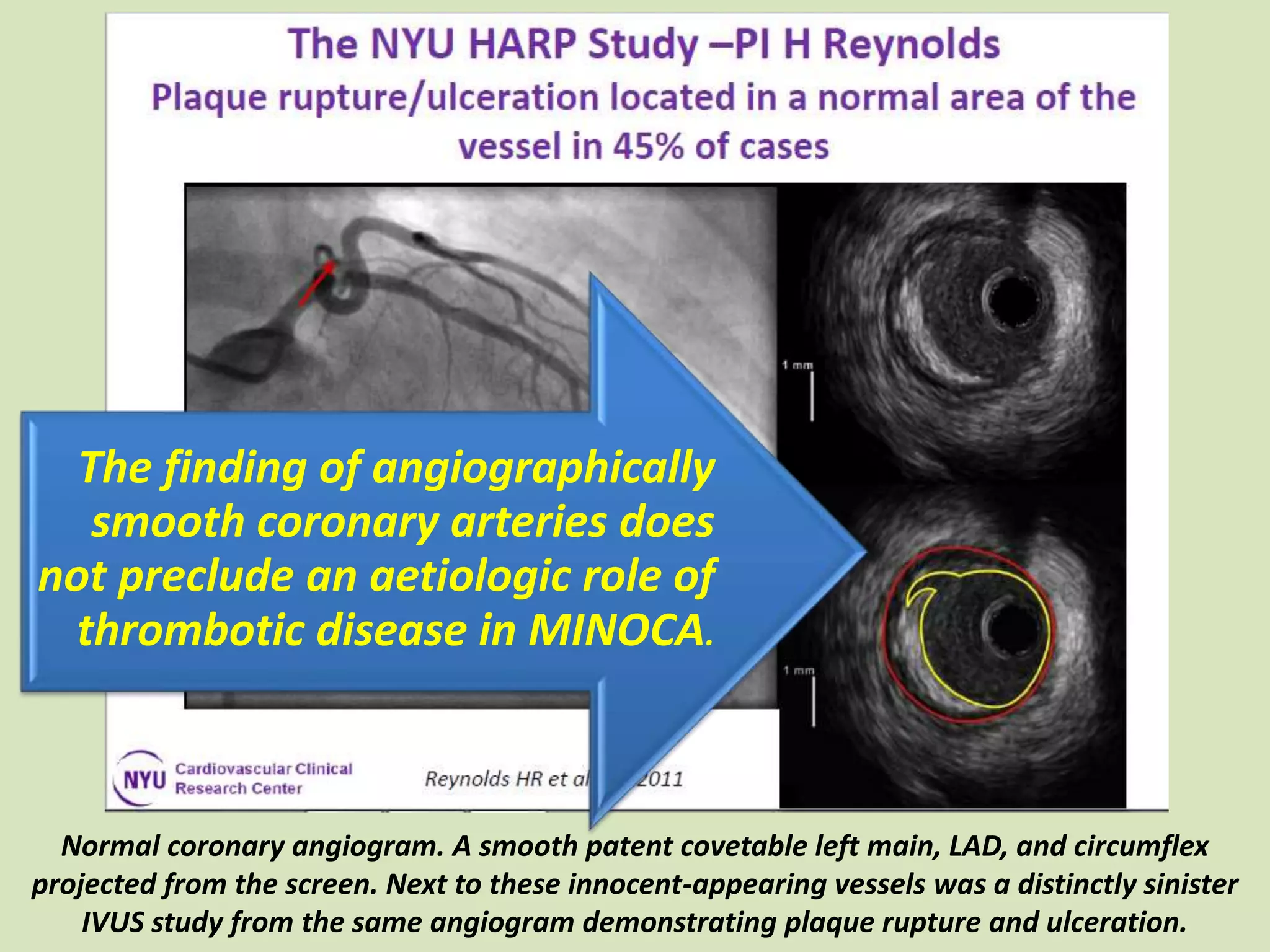
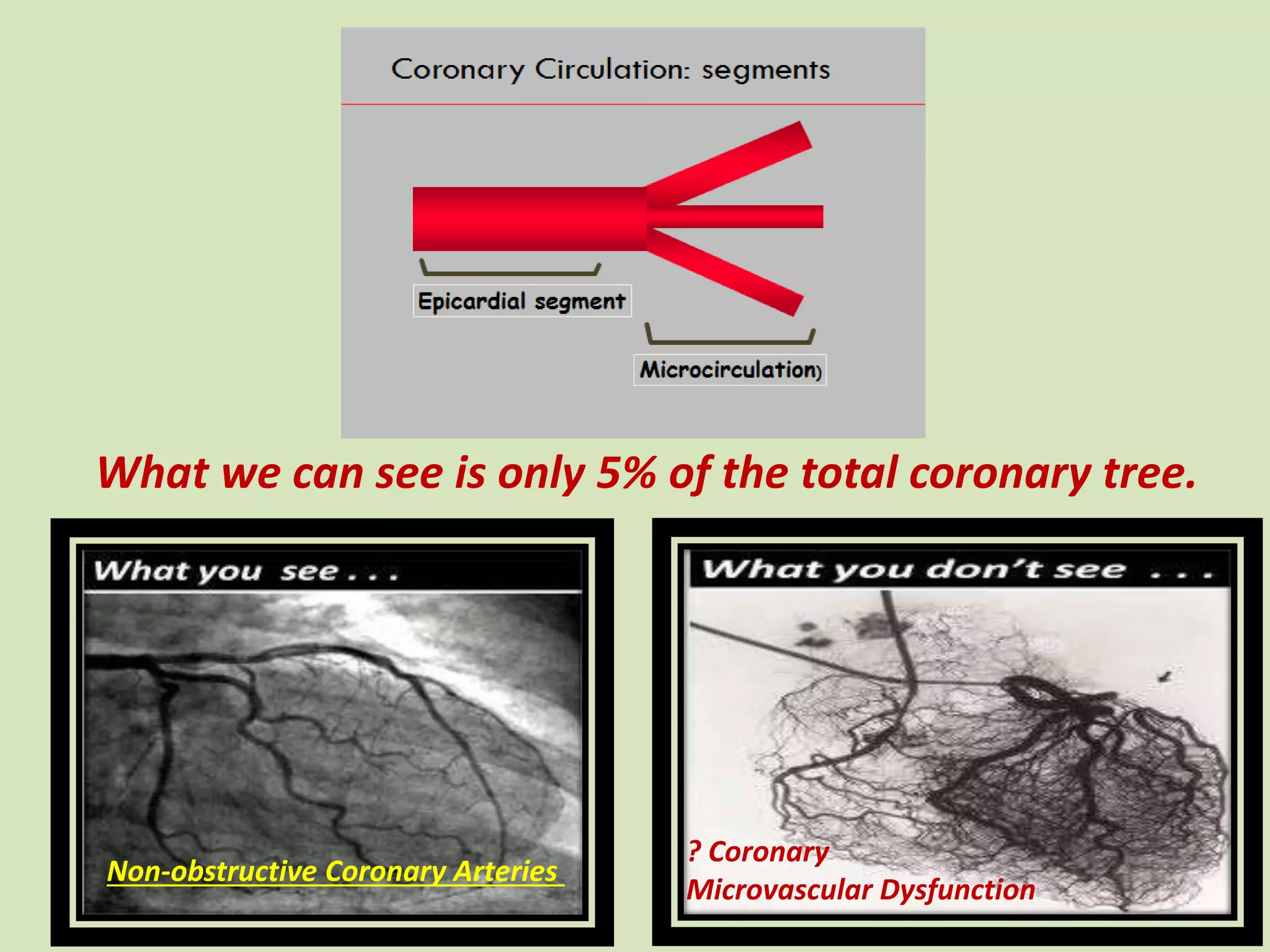
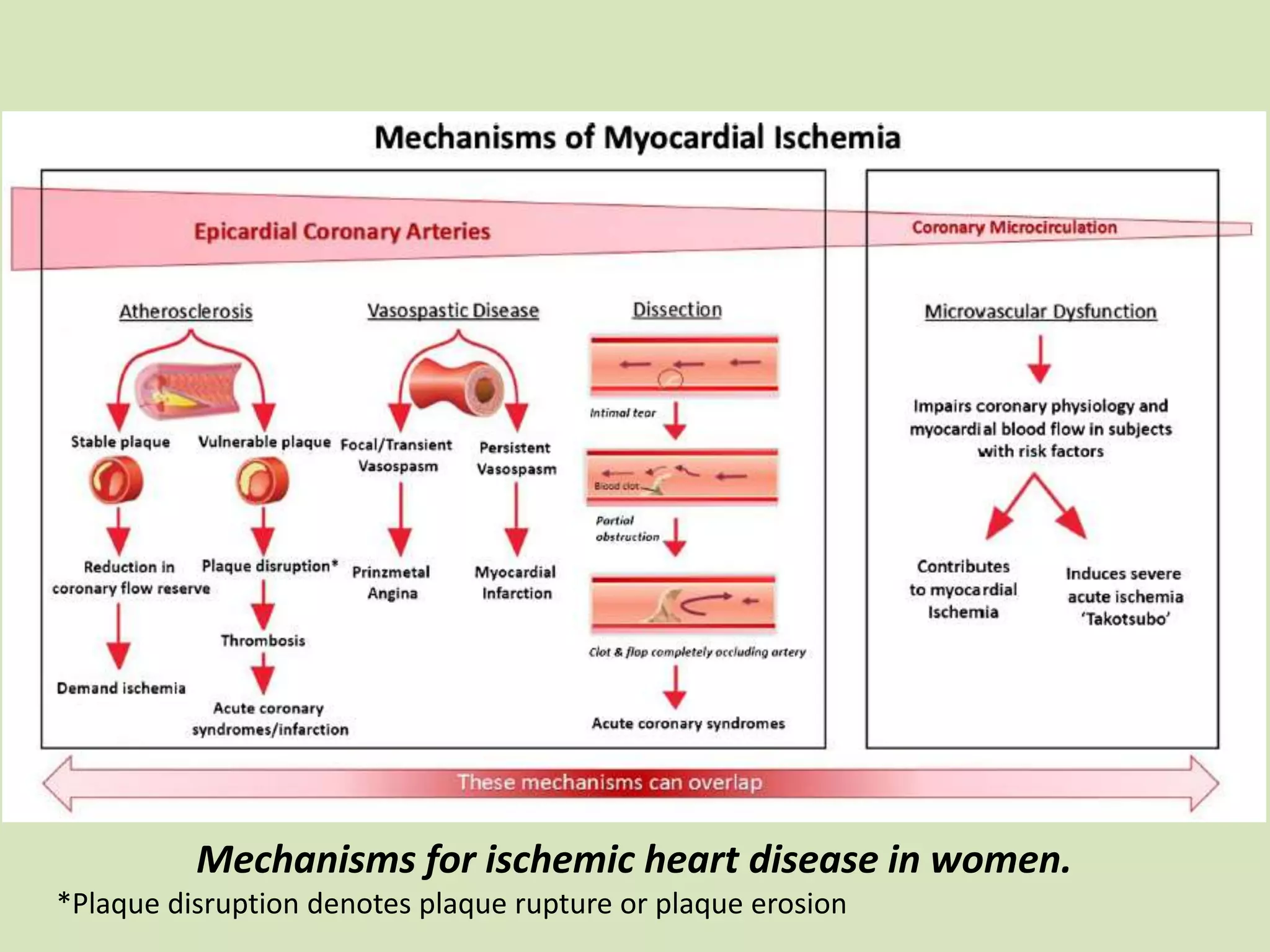
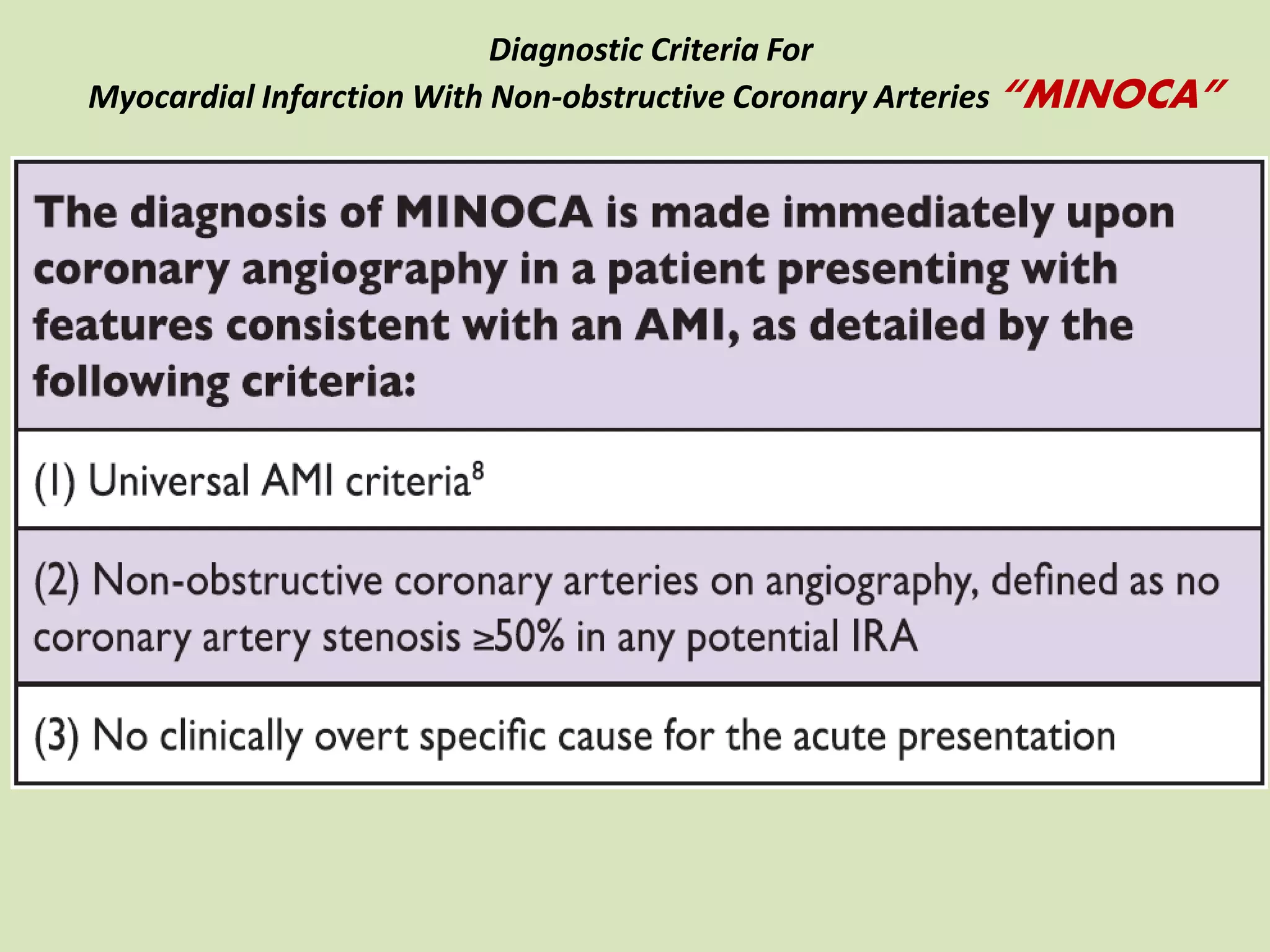
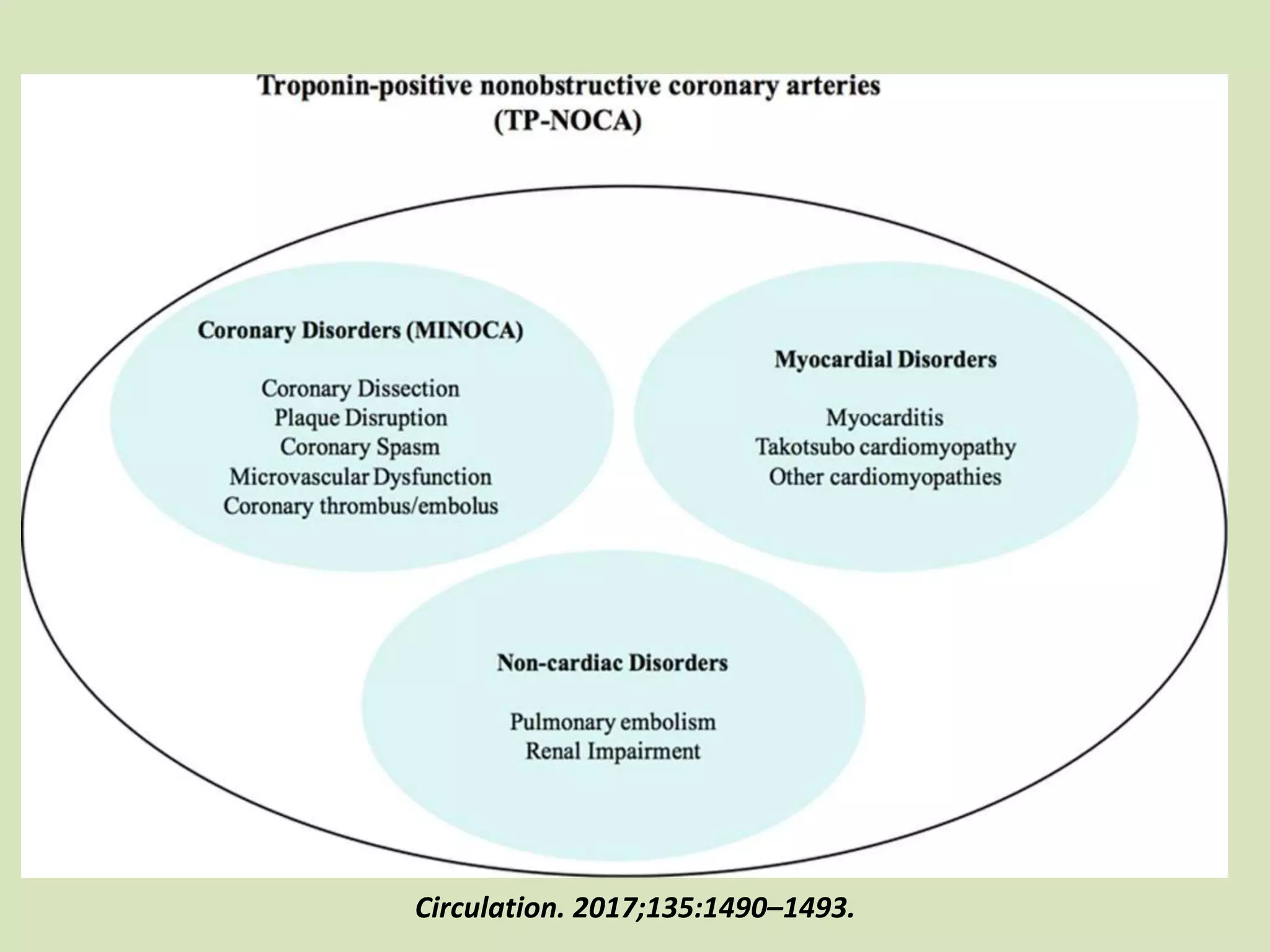
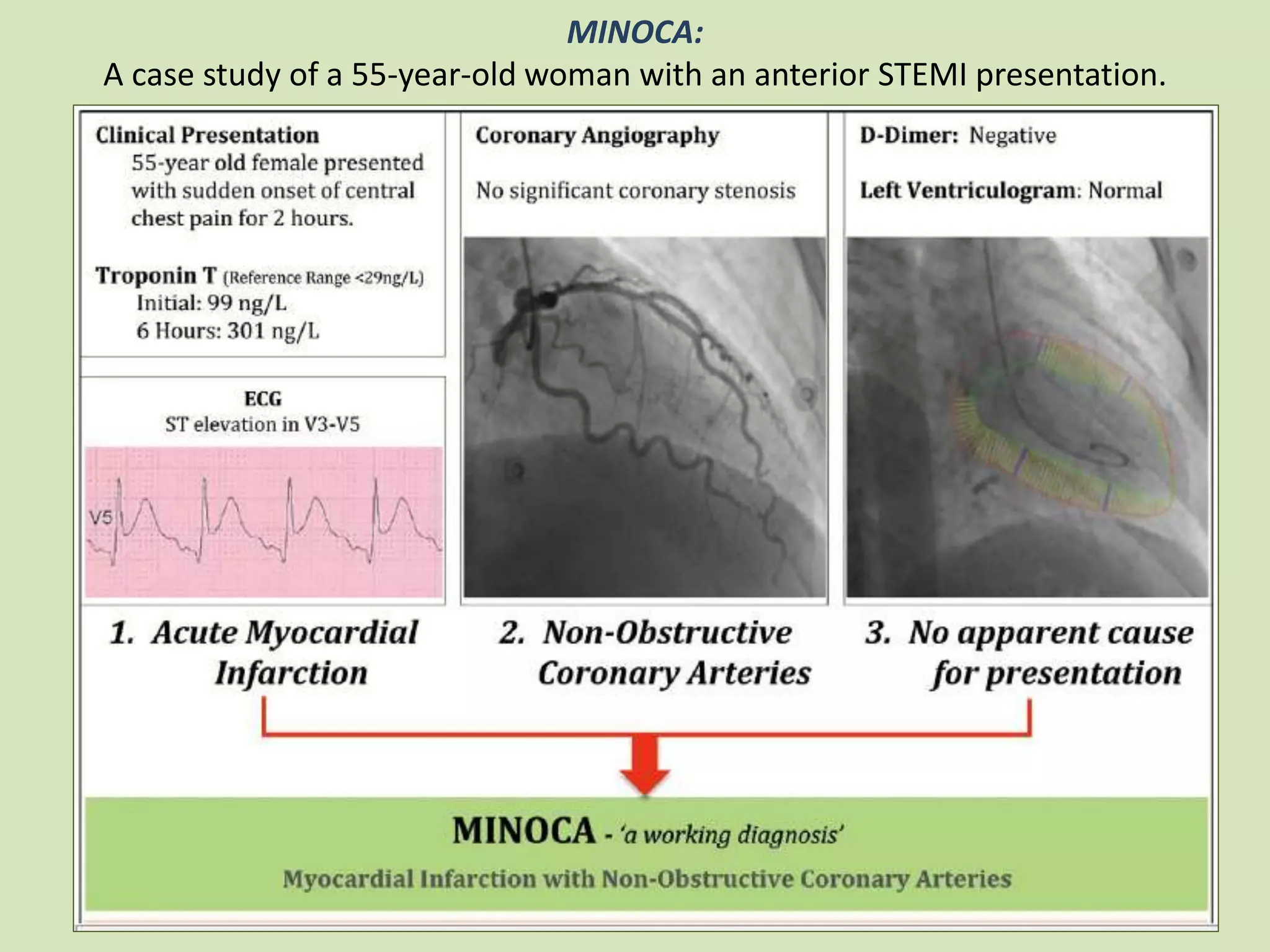
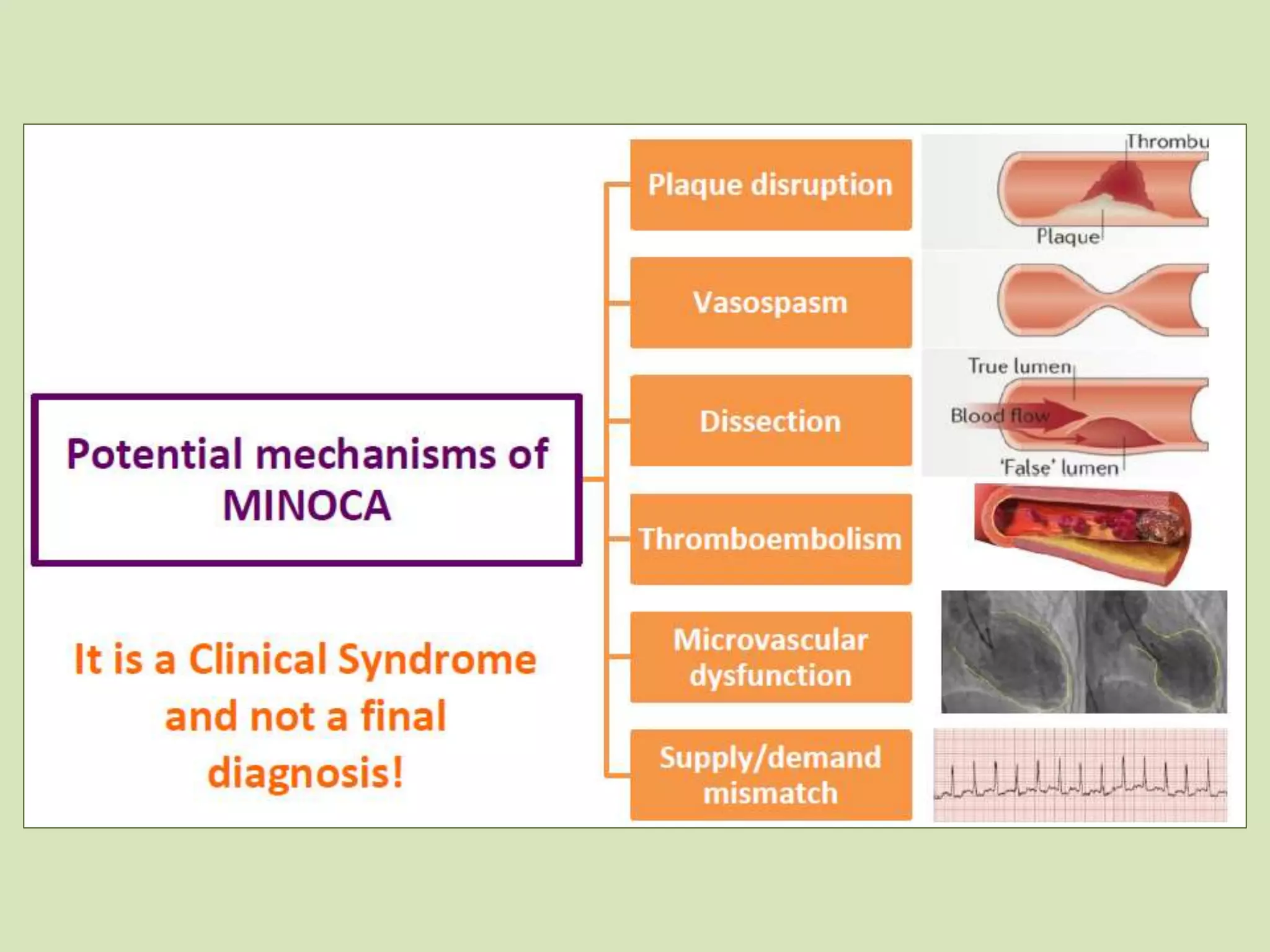
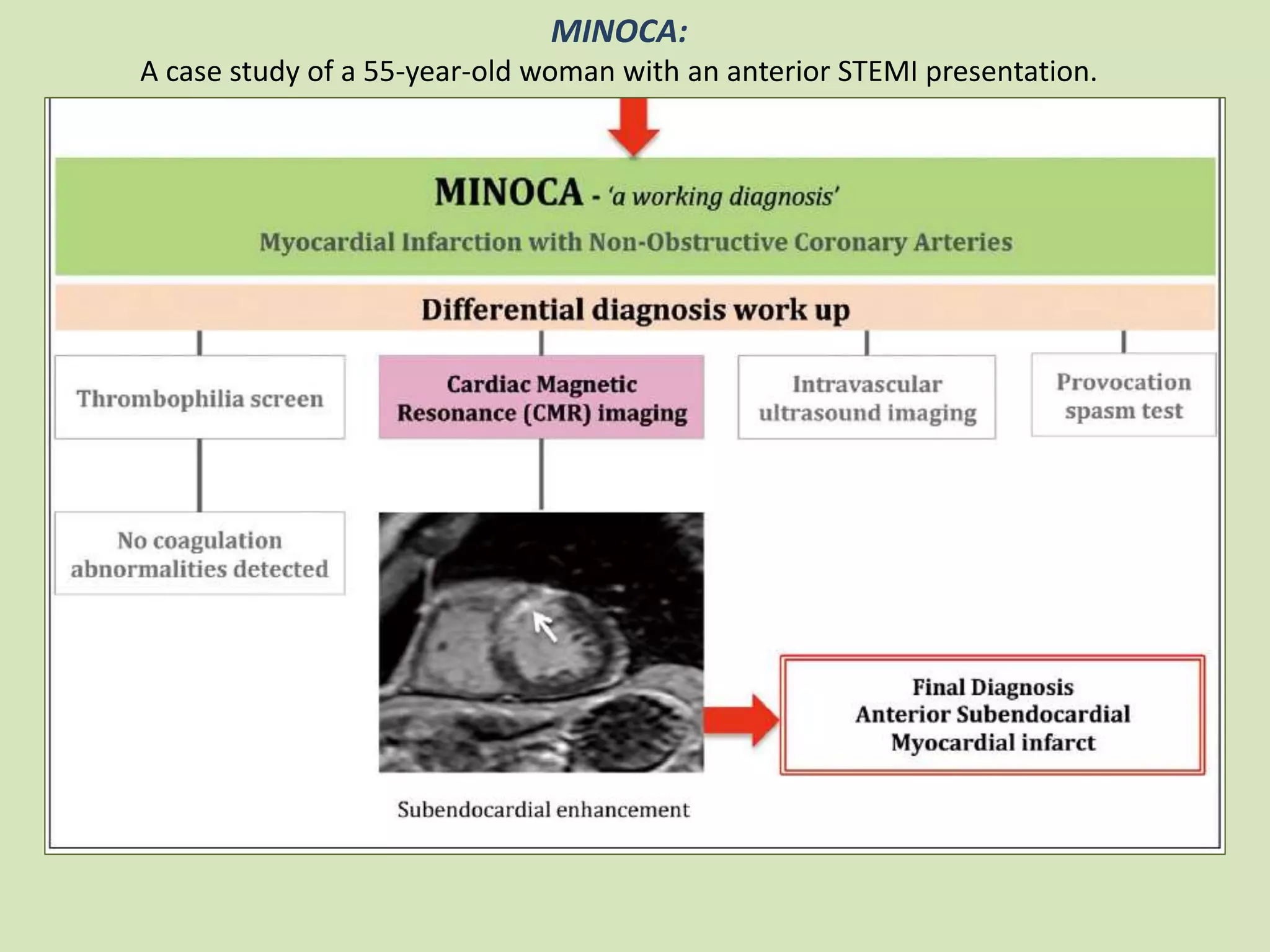
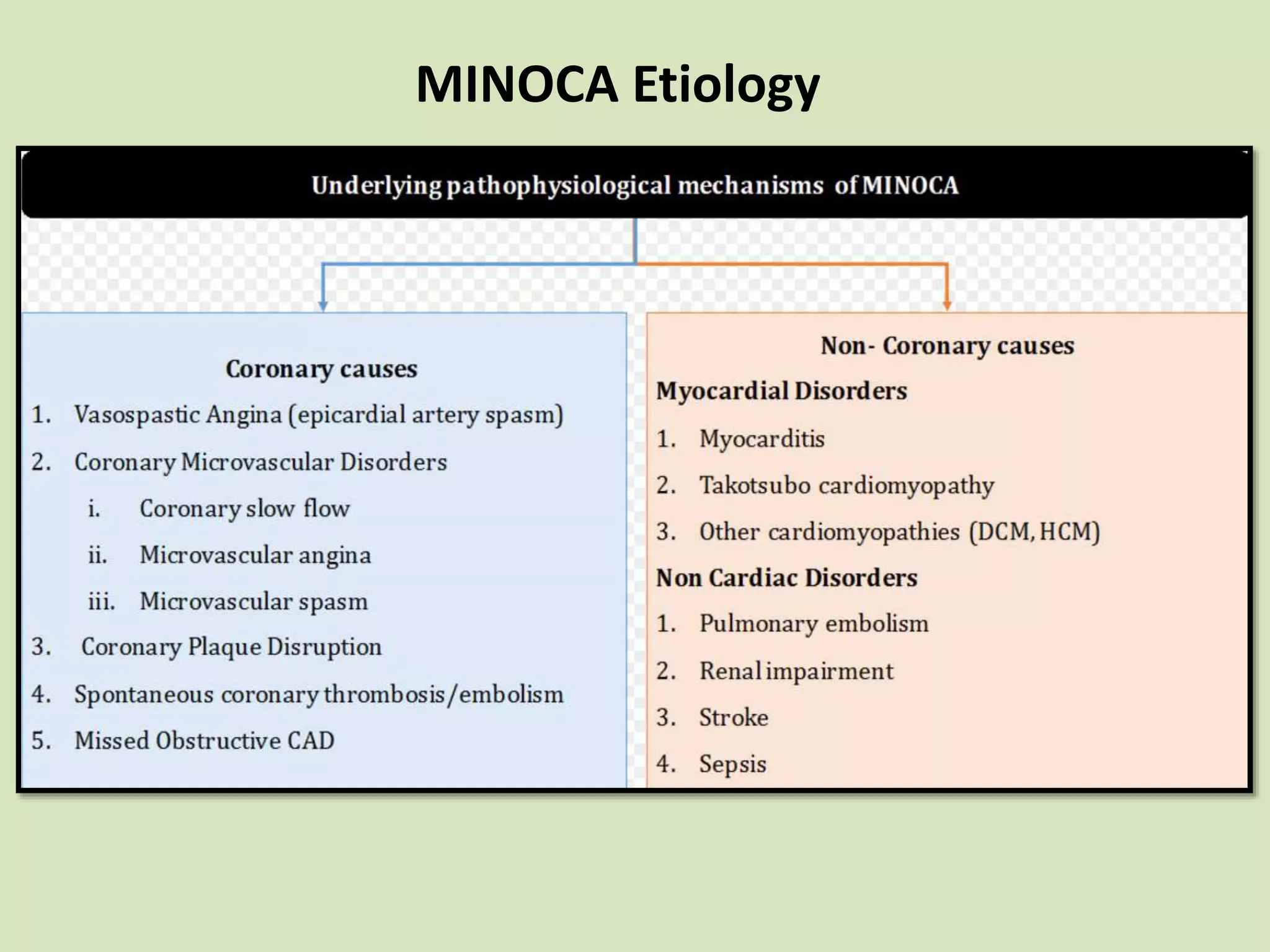
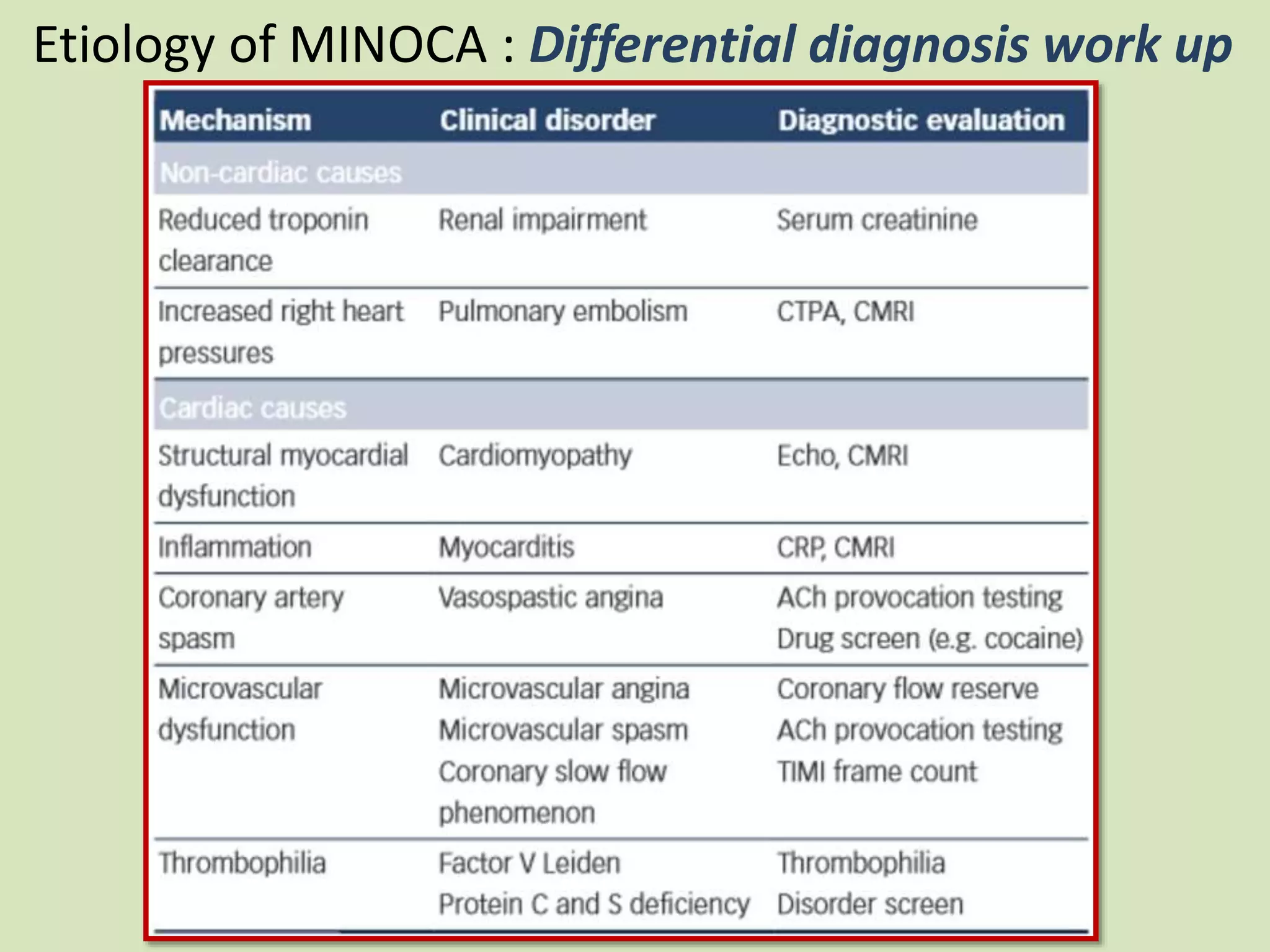
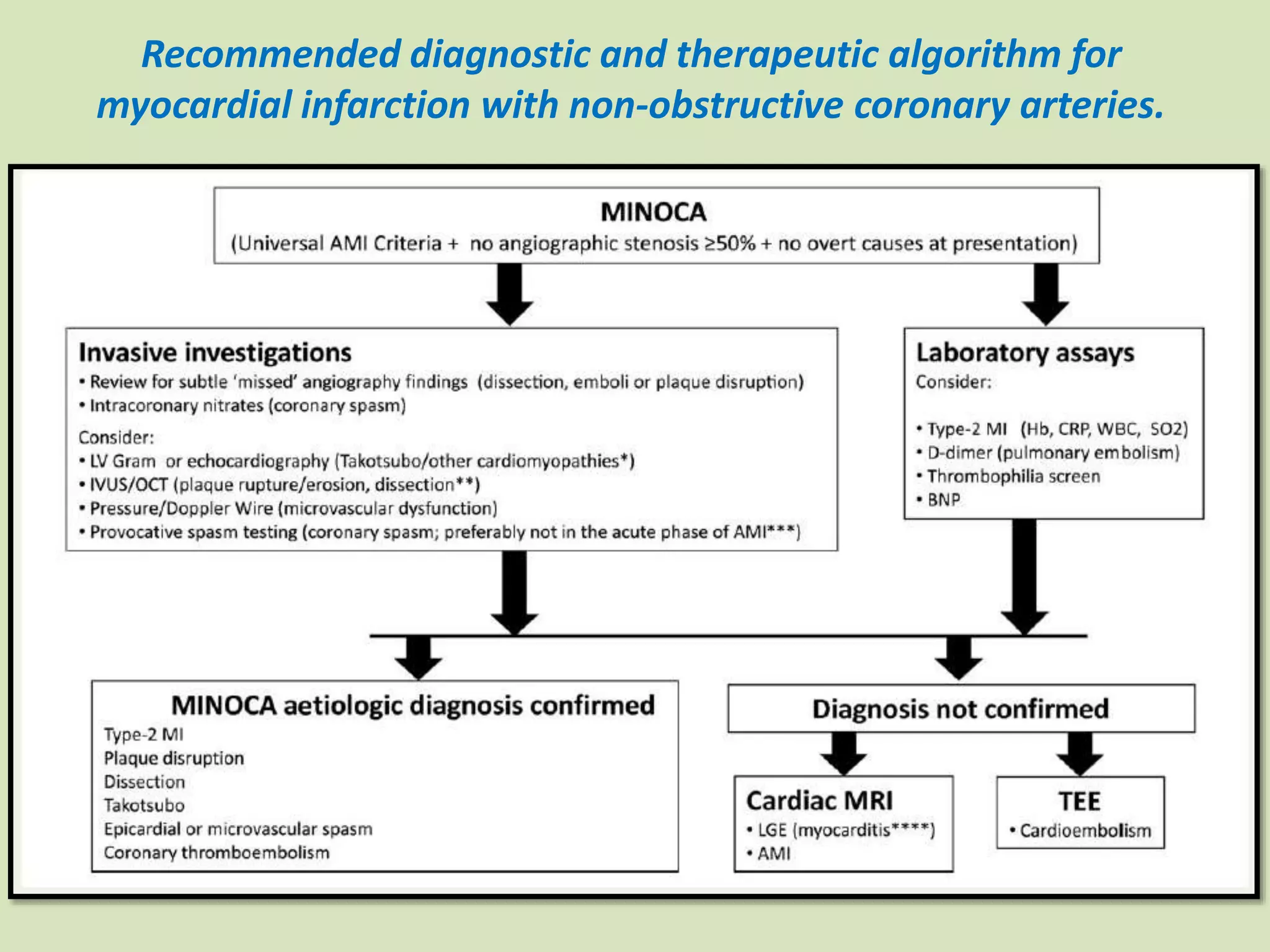
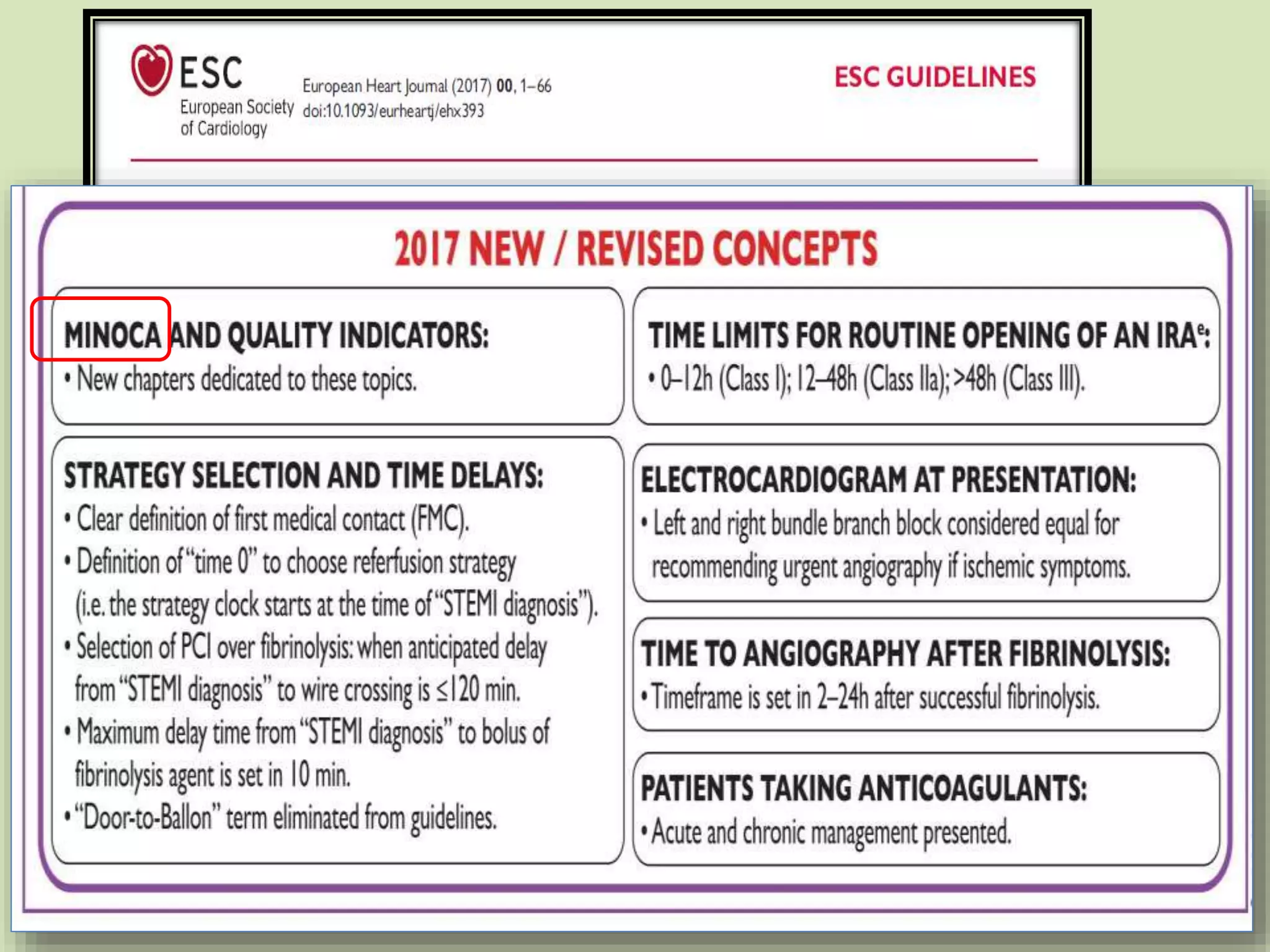
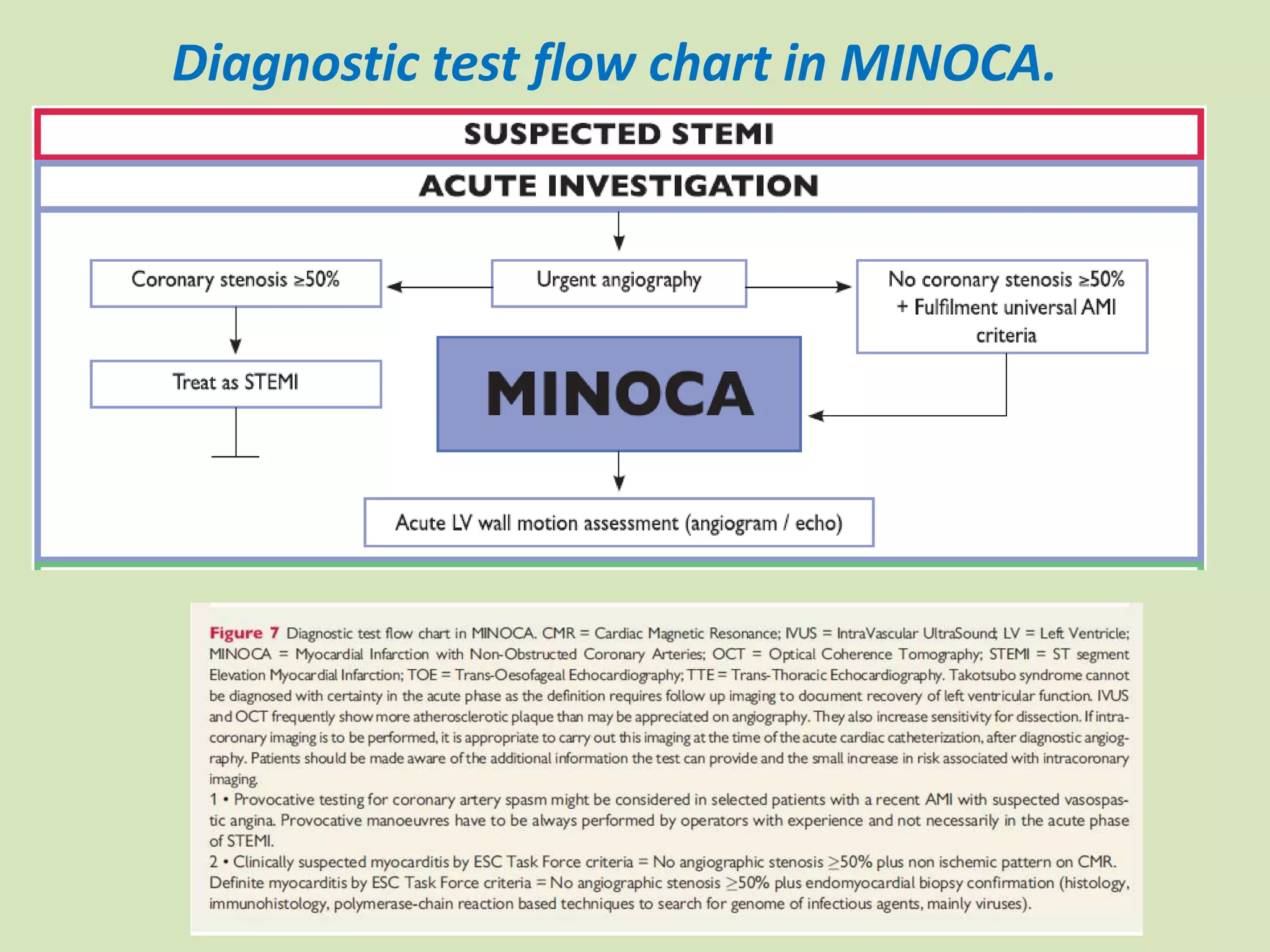
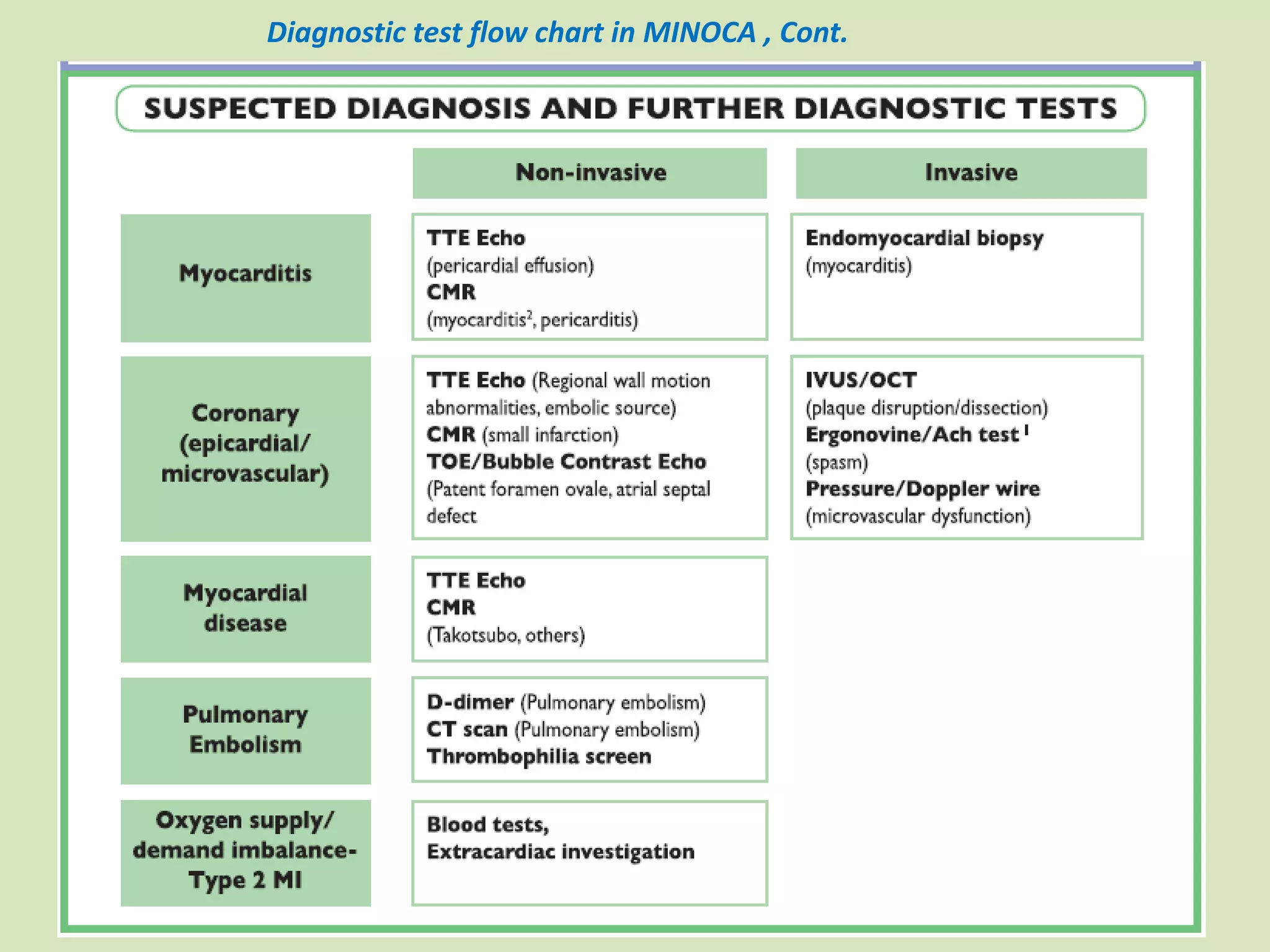
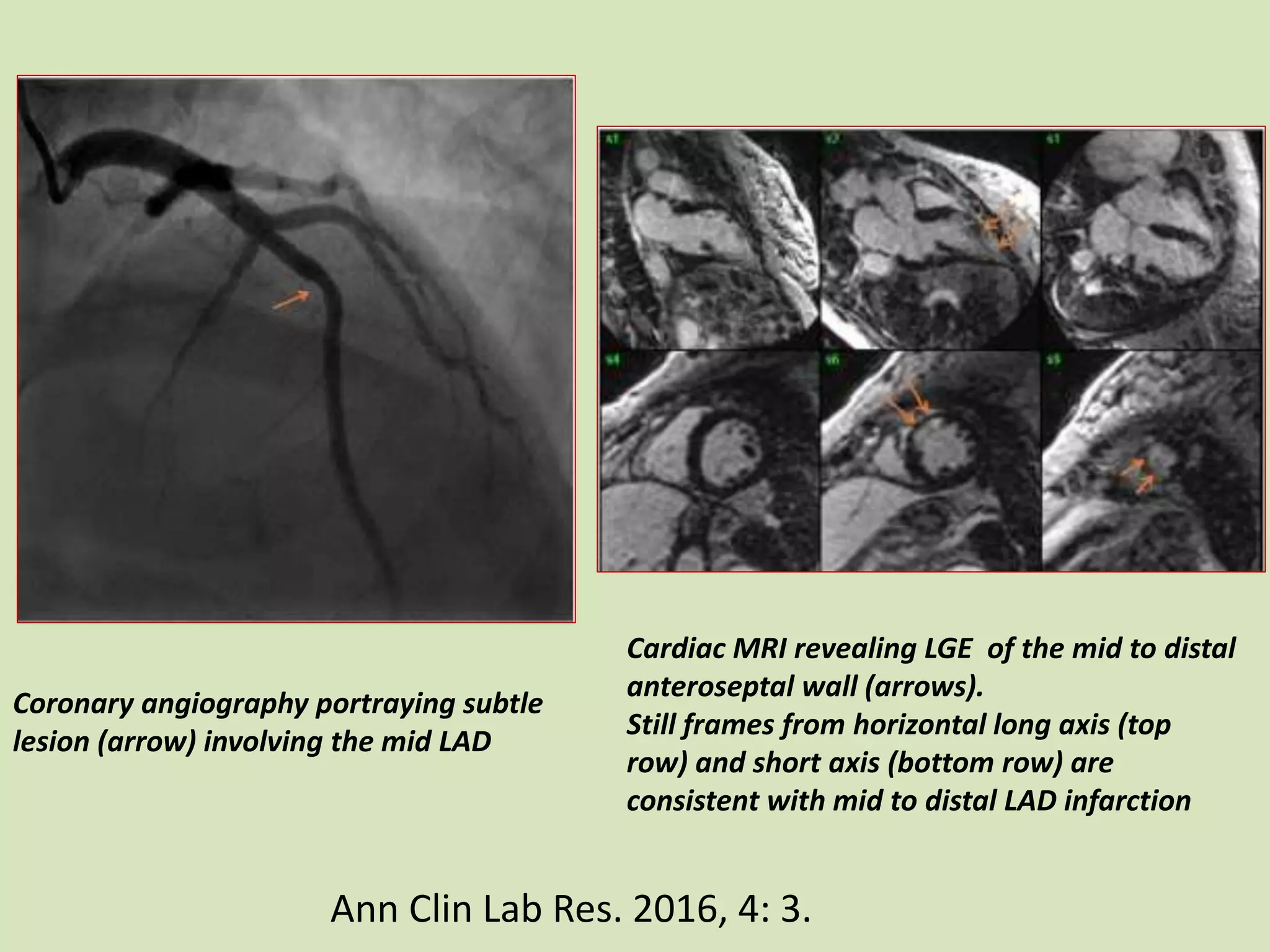
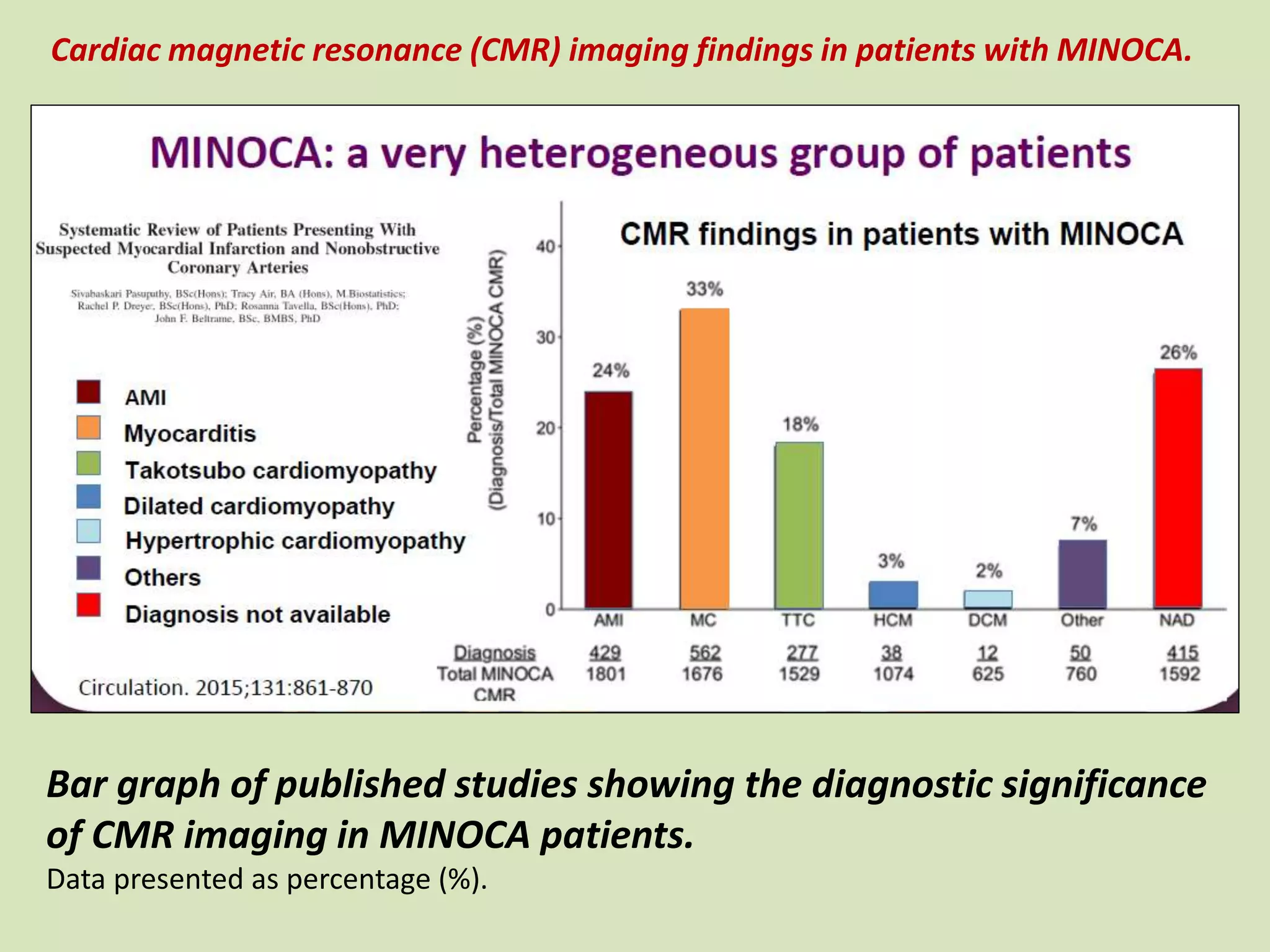
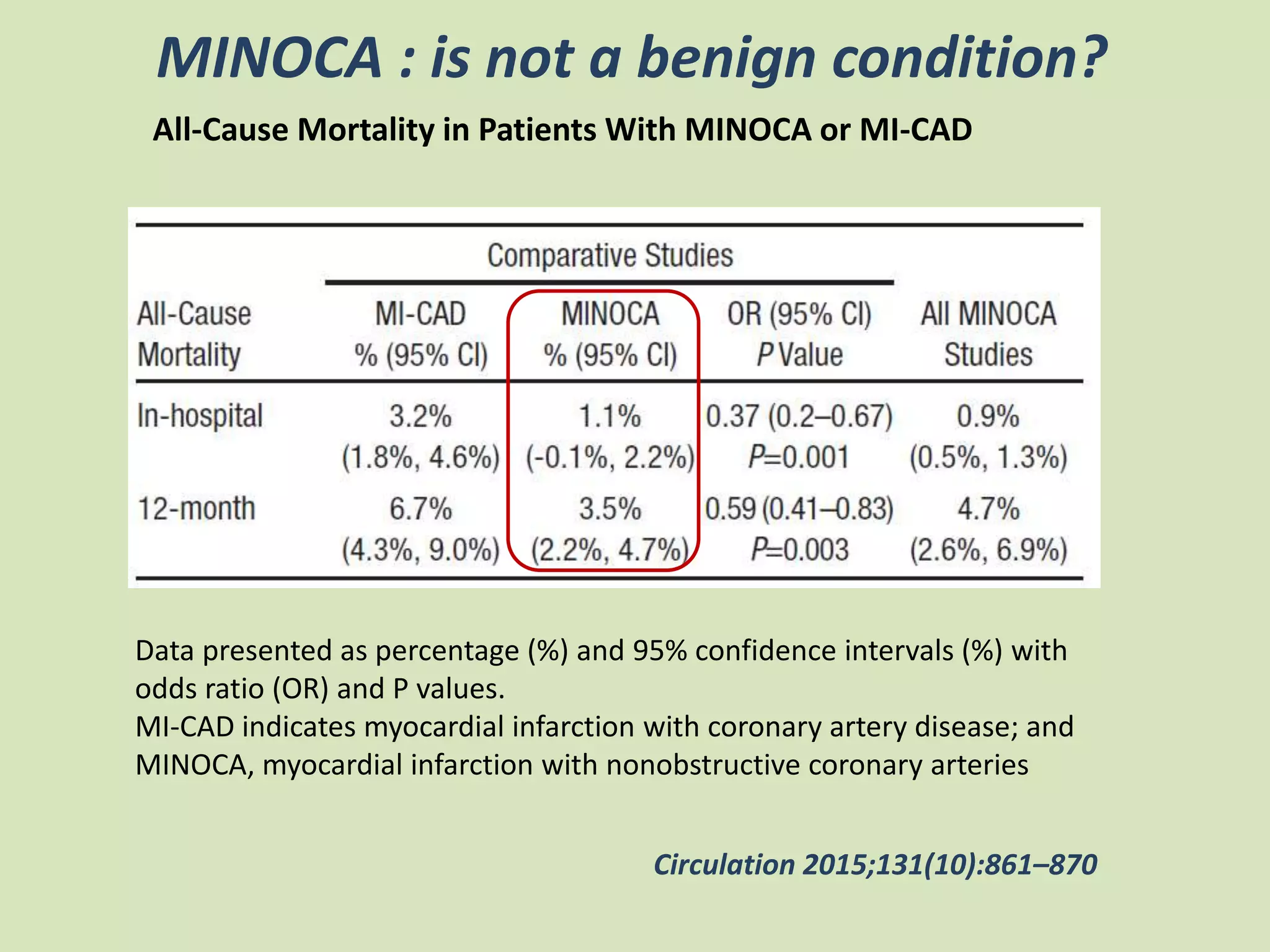
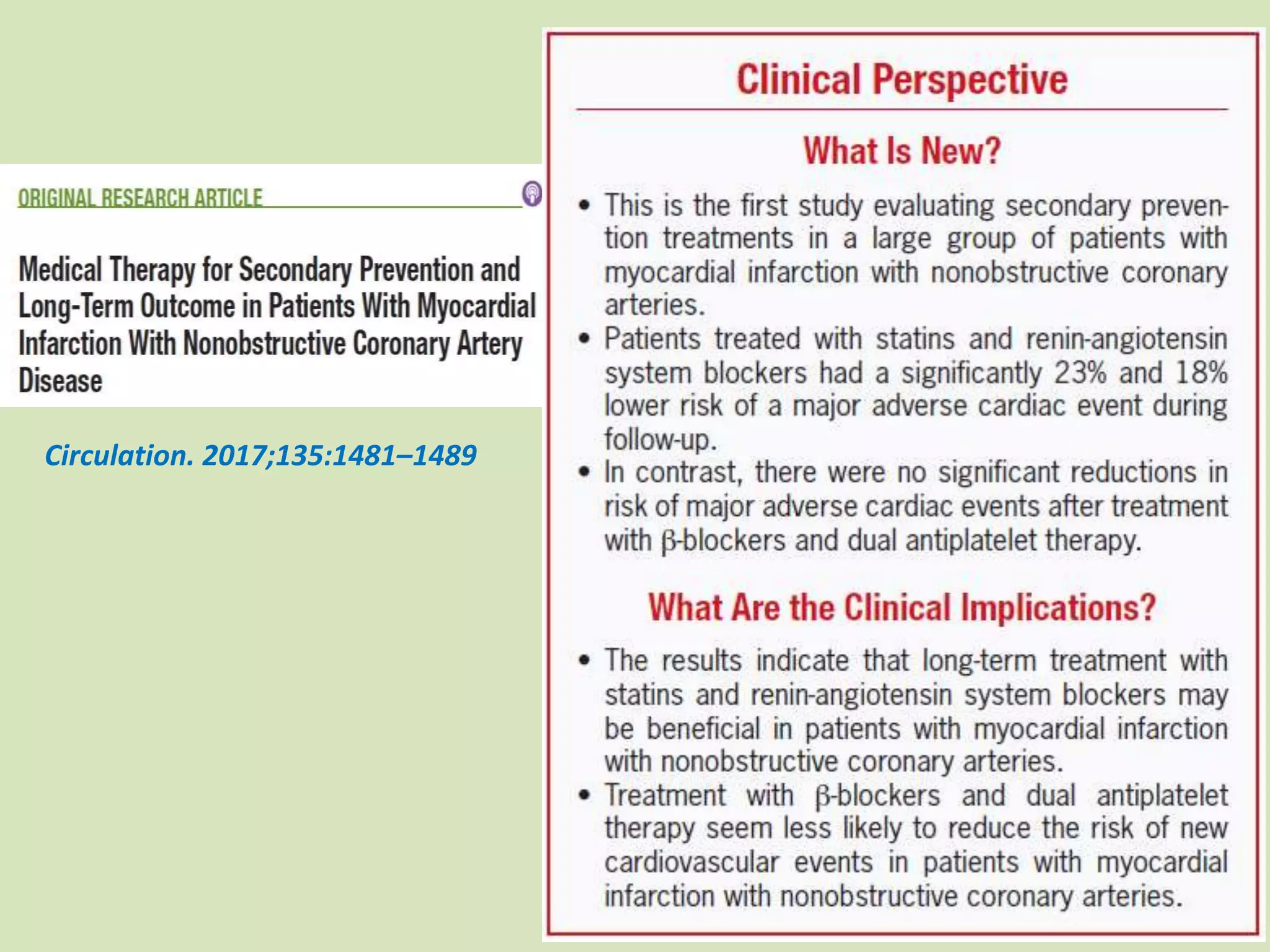
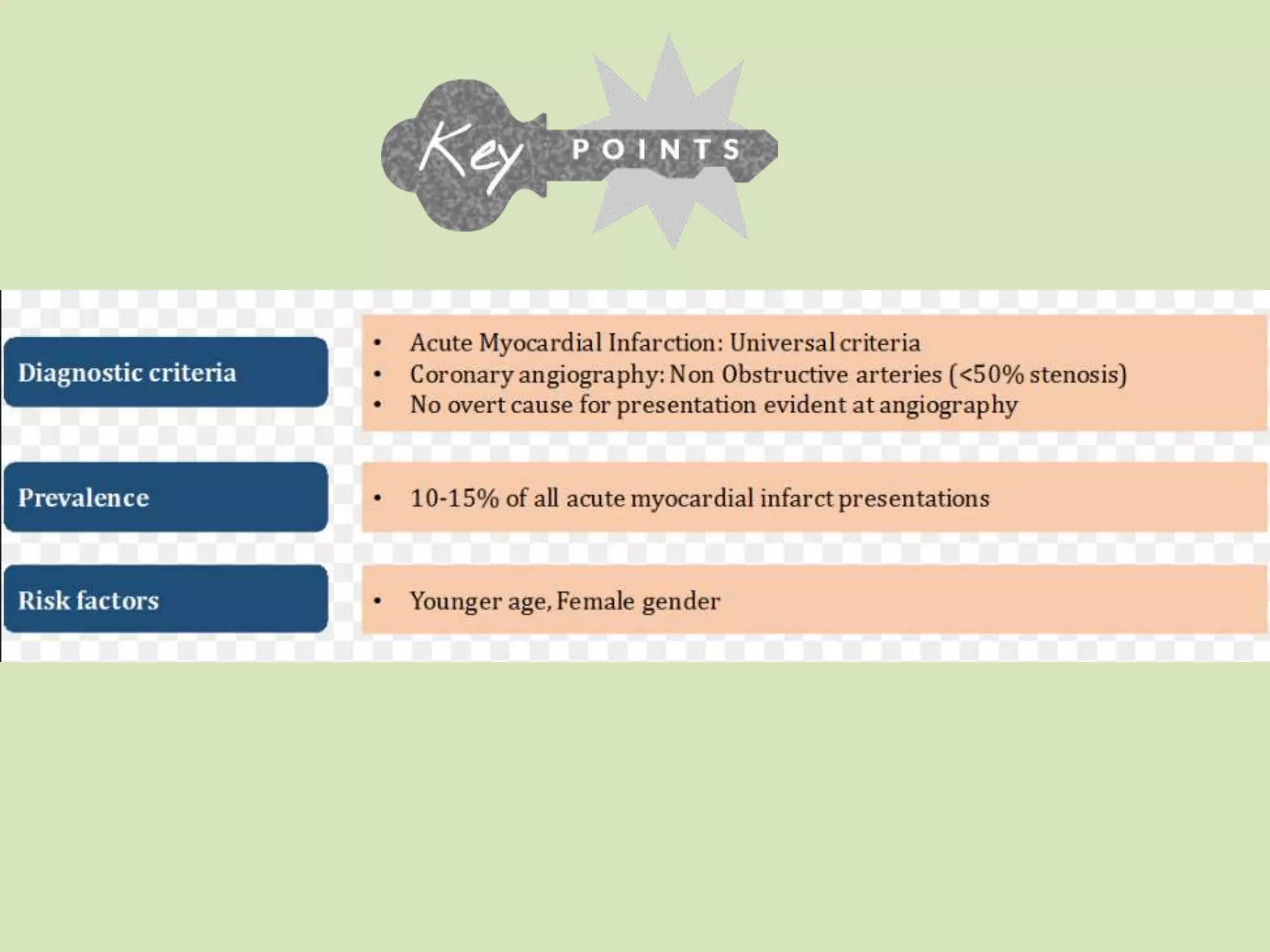

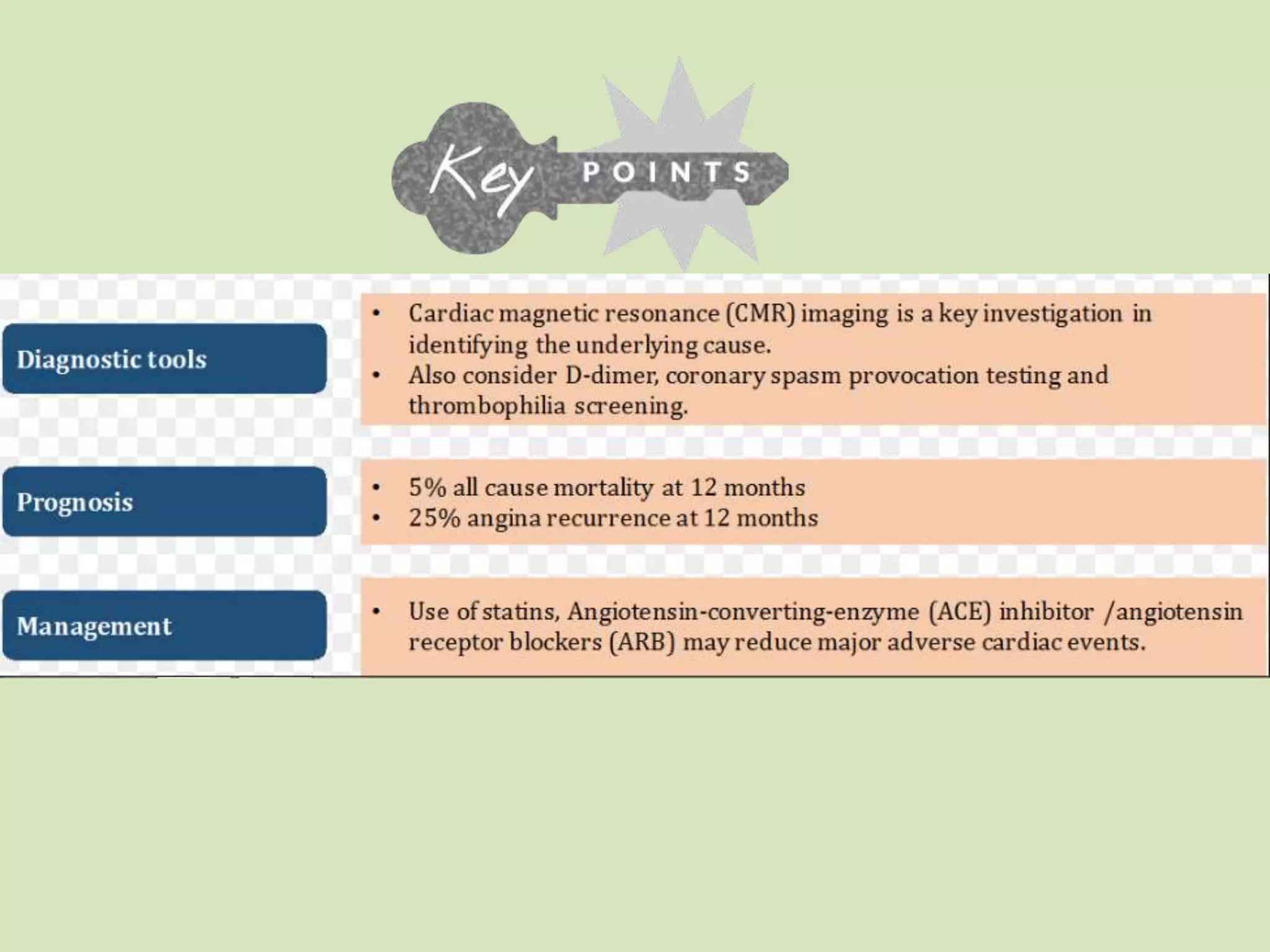
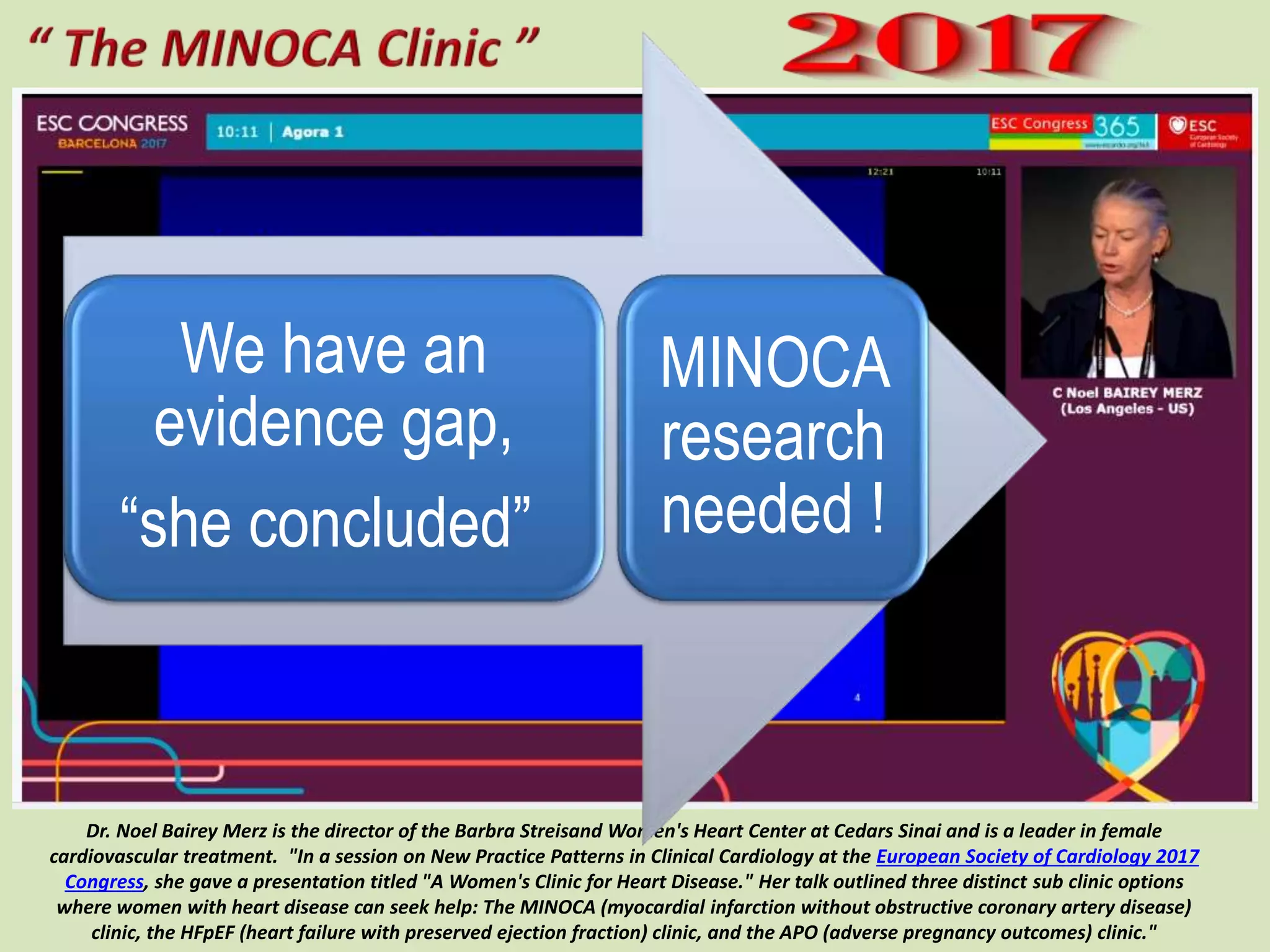


The document discusses the increasing recognition of myocardial infarction with non-obstructive coronary arteries (MINOCA) as a serious condition, highlighting its diagnostic complexities and the need for further investigation into its underlying causes. It emphasizes the importance of cardiac magnetic resonance imaging (CMR) in evaluating MINOCA and argues that it warrants the same clinical attention as myocardial infarction with obstructive coronary artery disease. The document also notes that patients with MINOCA have a significant one-year mortality risk, underscoring the necessity for comprehensive management and research in this area.










































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












