Downloaded 602 times
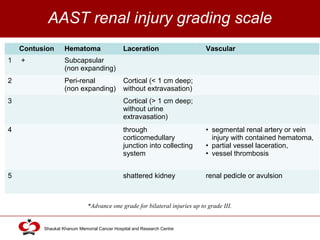
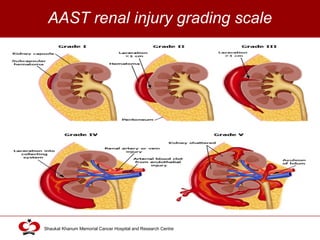



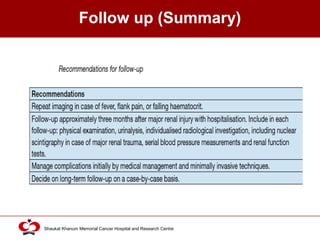
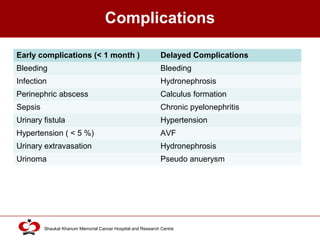
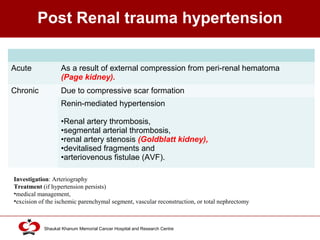
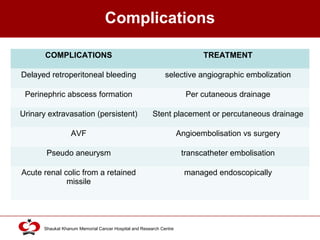
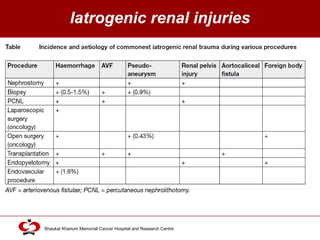
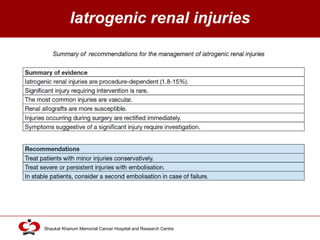
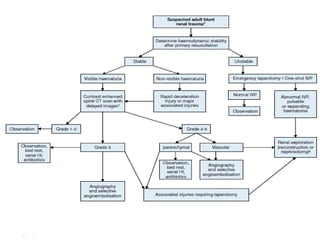
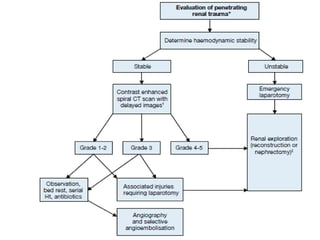


This document provides an overview of renal trauma, including epidemiology, modes of injury, classification systems, diagnostic evaluation, disease management, and complications. It discusses the American Association for the Surgery of Trauma renal injury grading scale and recommendations for initial patient evaluation, laboratory tests, and imaging modalities like CT, US, and IVP. Treatment options include conservative management with observation, angioembolization for bleeding injuries, and surgical exploration for hemodynamic instability or high-grade injuries. The goal is to control hemorrhage while salvaging the kidney through reconstruction when possible.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
