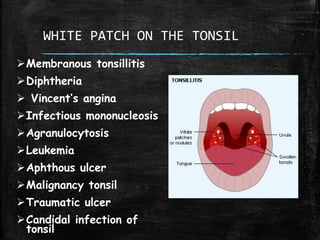
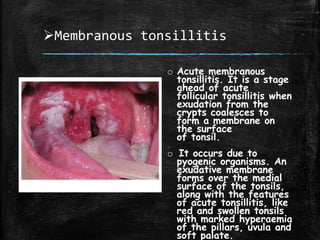
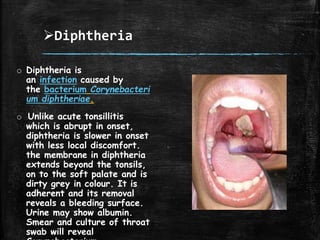
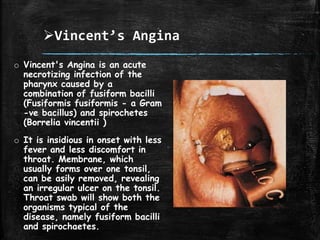
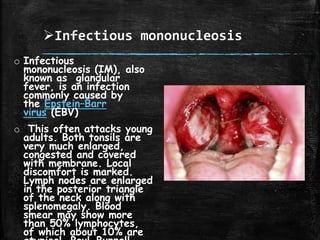
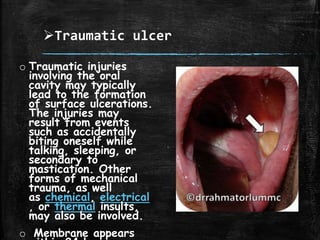
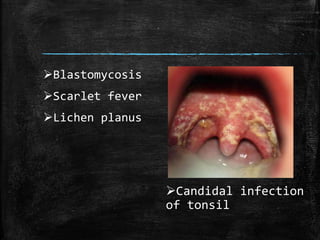
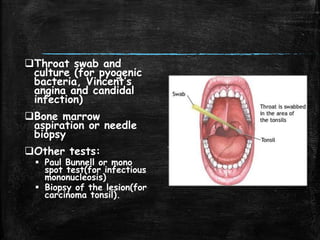
White patches on the tonsils can have several potential causes, including infections like strep throat, diphtheria, and mononucleosis. Other possible causes include conditions like agranulocytosis, leukemia, aphthous ulcers, and tonsil cancer. A thorough examination and tests are needed to determine the specific cause, which may involve a throat swab culture, blood tests, or biopsy of the affected area. Differential diagnosis requires considering both infectious and non-infectious potential etiologies.